ņä£ ļĪĀ
ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźś(extracranial carotid artery aneurysm)ļŖö ņĀäņ▓┤ ļÅÖļ¦źļźśņØś ņĢĮ 0.4~1% ņĀĢļÅäļ¦īņØä ņ░©ņ¦ĆĒĢśļŖö ļō£ļ¼Ė ņ¦łĒÖśņ£╝ļĪ£, ļÅÖļ¦źĻ▓ĮĒÖöņ”ØņØ┤ Ļ░Ćņן ĒØöĒĢ£ ņøÉņØĖņØ┤ļŗż[1]. ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźśļŖö ĒŖ╣ļ│äĒĢ£ ņ”ØņāüņŚåņØ┤ ļ░£Ļ▓¼ļÉśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ņ£╝ļéś, ļ░ĢļÅÖņä▒ Ļ▓ĮļČĆņóģļ¼╝ņØ┤ļéś ļćīĻ▓Įņāē, ļćīņŗĀĻ▓Į ļ¦łļ╣ä, ĒśĖļäł ņ”ØĒøäĻĄ░(HornerŌĆÖs syndrome) ļō▒ņØś ņŗĀĻ▓ĮĒĢÖņĀü ņ”Øņāüņ£╝ļĪ£ ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░Ļ░Ć ĒØöĒĢśļŗż[2]. ĻĄ¼Ļ░Ģ ļé┤ ņóģĻ┤┤ļ¦īņ£╝ļĪ£ ļ░£Ļ▓¼ļÉśļŖö Ļ▓ĮņÜ░ļŖö ļō£ļ¼╝ļ®░, ņØ┤ ņżæ ļ░£ņŚ┤ņØ┤ļéś ņŚ╝ņ”ØņåīĻ▓¼ņØ┤ ļÅÖļ░śļÉśņ¢┤ ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņ£╝ļĪ£ ņśżņØĖļÉ£ Ļ▓ĮņÜ░ļŖö ļŹö ļō£ļ¼╝ņ¢┤ Ēśäņ×¼Ļ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ ļ¼ĖĒŚīņØ┤ ļ¦żņÜ░ ņĀüĻ│Ā[3-5], ĻĄŁļé┤ņŚÉņä£ļŖö ņĢäņ¦üĻ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ ļ░ö ņŚåļŗż. ņĀĆņ×ÉļŖö ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņ£╝ļĪ£ ņśżņØĖļÉśņŚłļŹś ļæÉĻ░£ņÖĖ ļé┤Ļ▓ĮļÅÖļ¦źļźś(extracranial internal carotid artery aneurysm) 1ņśłļź╝ Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”Ø ļĪĆ
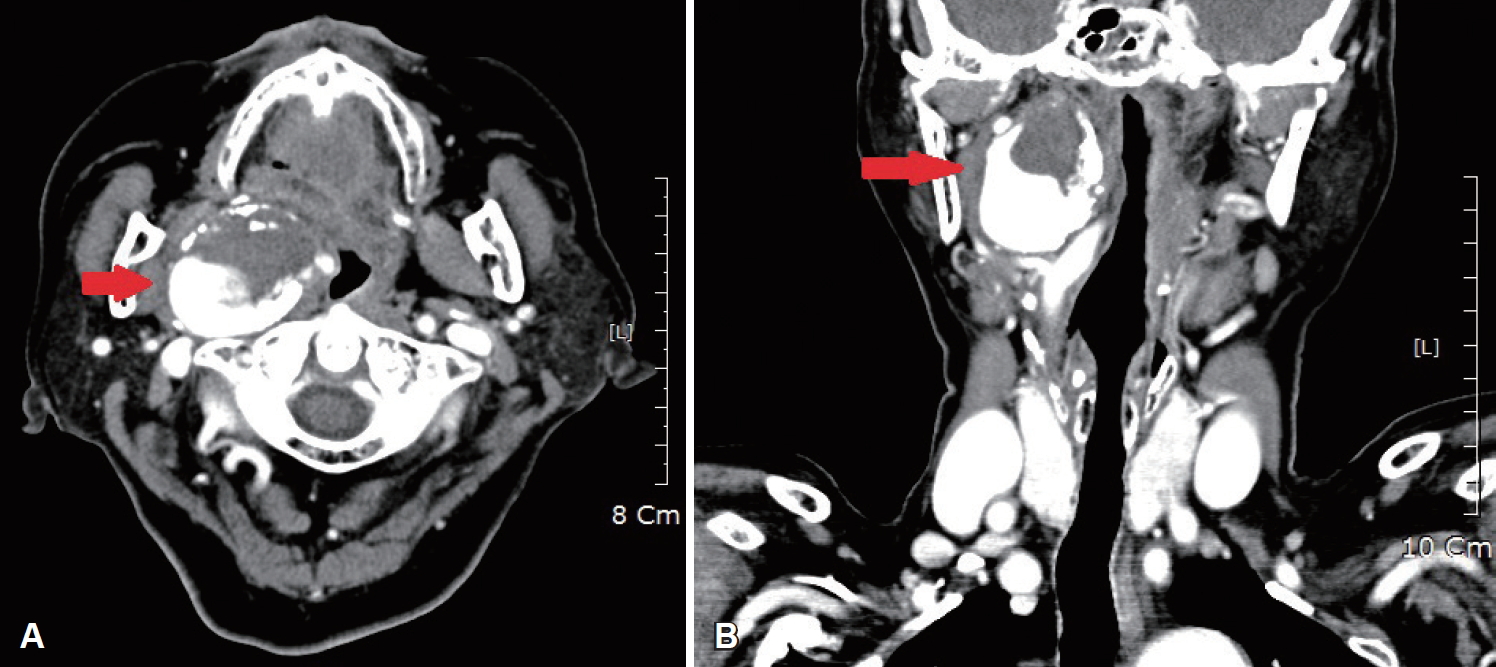
81ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉĻ░Ć ņØ╝ņŻ╝ņØ╝ ņĀäļČĆĒä░ ņä£ņä£Ē׳ ņĢģĒÖöļÉ£ Ļ│ĀņŚ┤, ņĀäņŗĀ ĻĘ╝ņ£ĪĒåĄ ļ░Å ņØĖĒøäĒåĄņØä ņŻ╝ņåīļĪ£ ņÖĖļלņŚÉ ļé┤ņøÉĒĢśņśĆļŗż. ĒÖśņ×ÉļŖö Ļ░£ņØĖņØśņøÉņŚÉņä£ Ļ▓ĮĻĄ¼ņĢĮņØä ļ│ĄņÜ®ĒĢśņśĆņ£╝ļéś ņ”ØņäĖĻ░Ć ĒśĖņĀäļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ņÜ░ņĖĪ ĒÄĖļÅäņŻ╝ņ£ä ņóģņ░Įņ£╝ļĪ£ ņØśļó░ļÉśņŚłļŗż. ĻĖ░ņĀĆņ¦łĒÖśņ£╝ļĪ£ Ļ│ĀĒśłņĢĢņŚÉ ļīĆĒĢ£ Ļ▓ĮĻĄ¼ņĢĮ ļ│ĄņÜ® ņÖĖņŚÉļŖö ĒŖ╣ņØ┤ņé¼ĒĢŁņØ┤ ņŚåņŚłņ£╝ļ®░, ĻĘĖ ņÖĖ ĒÄĖļÅäņĀłņĀ£ņłĀņØä ĒżĒĢ©ĒĢ£ ņłśņłĀļĀź, ņÖĖņāü, ĒśłĻ┤ĆĻ│╝ Ļ┤ĆļĀ©ĒĢ£ ņŗ£ņłĀ ļō▒ņØś Ļ│╝Ļ▒░ļĀźņØĆ ņŚåņŚłļŗż. ļé┤ņøÉ ļŗ╣ņŗ£ 38.1┬░CņØś ļ░£ņŚ┤ņØ┤ ņ׳ņŚłņ£╝ļ®░, ņŗ£Ē¢ēĒĢ£ ĒśłņĢĪĻ▓Ćņé¼ņāü Ēśłņżæ ļ░▒ĒśłĻĄ¼ ņłśņ╣ś 18.30├Ś103/╬╝L, ESR 102 mm/hr, C-reactive protein 25.49 mg/dLļĪ£ ņŚ╝ņ”Øņłśņ╣ś ļśÉĒĢ£ ņāüņŖ╣ļÉśņ¢┤ ņ׳ņŚłļŗż. ņŗ£Ē¢ēĒĢ£ ņŗĀņ▓┤Ļ▓Ćņ¦äņāü ņÜ░ņĖĪ ĒÄĖļÅäņÖĆ ņŻ╝ņ£äņØś ņŚ░ĻĄ¼Ļ░£ņŚÉ ņóģņ░Į ļ░Å ļ░£ņĀü ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░, ĻĄ¼Ļ░£ņłśņØś ņóīņĖĪ ĒÄĖņ£ä ņåīĻ▓¼ļ│┤ņØ┤Ļ│Ā ņ׳ņŚłĻ│Ā(Fig. 1), Ļ▓ĮļČĆ ļČĆņóģņØ┤ļéś ņóģĻ┤┤ ļō▒ņØś ņåīĻ▓¼ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļ®░, ļŗżļźĖ ņŗĀĻ▓ĮĒĢÖņĀü ņ”ØņāüļÅä ņŚåņŚłļŗż.
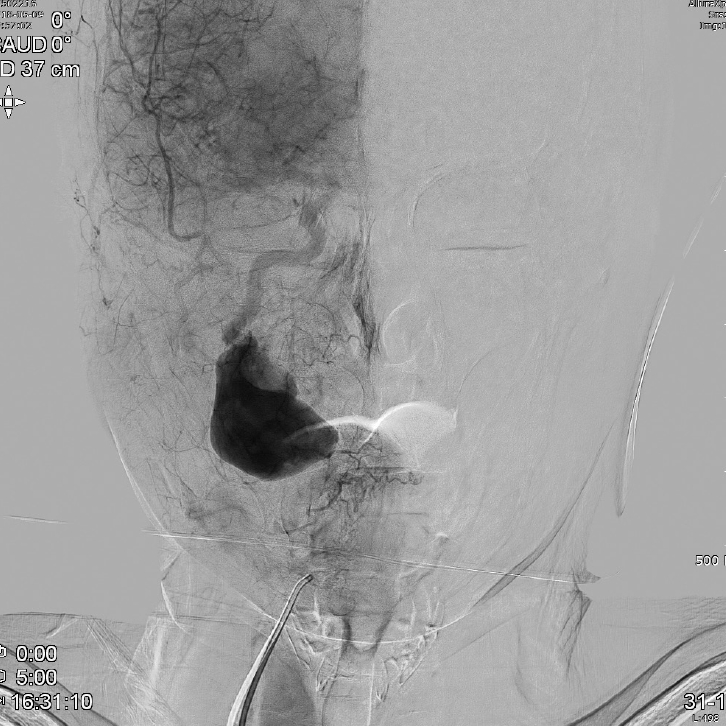
ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņØä ņØśņŗ¼ĒĢśņśĆņ£╝ļéś ĻĄ¼Ļ░Ģļé┤ ņ▓£ņ×Éļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖĻ│Ā, Ļ▓ĮļČĆ ņĪ░ņśüņ”ØĻ░Ģ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśüņØä ļ©╝ņĀĆ ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, ņÜ░ņĖĪ ļé┤Ļ▓ĮļÅÖļ¦źņØś ĻĘ╝ņ£äļČĆņŚÉ ĒśłņĀäņØ┤ ļÅÖļ░śļÉ£ ņ¦üĻ▓Į 5 cm Ēü¼ĻĖ░ņØś ņĪ░ņśü ņ”ØĻ░ĢļÉśļŖö ļÅÖļ¦źļźśĻ░Ć ĻĄ¼ņØĖļæÉņ¬Įņ£╝ļĪ£ ļÅīņČ£ļÉ£ ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 2). ĒĢ┤ļŗ╣ ļ│æļ│ĆņŚÉ ļīĆĒĢ┤ ņŗĀĻ▓ĮņÖĖĻ│╝ Ēśæņ¦äņØä ņØśļó░ĒĢśņśĆĻ│Ā, ļīĆĒć┤ļÅÖļ¦źĻ▓Įņ£Ā ļćīĒśłĻ┤ĆņĪ░ņśüņłĀņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, ņÜ░ņĖĪ ņżæĻ▓ĮļČĆ(midcervical) ļé┤Ļ▓ĮļÅÖļ¦źņŚÉ ņĢĮ 4.9├Ś4.2├Ś3.8 cm Ļ░Ćļ¤ēņØś ĒśłņĀäņØä ļÅÖļ░śĒĢ£ ļÅÖļ¦źļźś ņåīĻ▓¼ņØä ļ│┤ņśĆĻ│Ā, ņØ┤ņÖĖ ņóīņĖĪ ļé┤Ļ▓ĮļÅÖļ¦ź ļ░Å ņ▓ÖņČöļÅÖļ¦źņŚÉ ņØ┤ņāü ņåīĻ▓¼ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 3).
ĒÖśņ×ÉņØś ļ░£ņŚ┤ņØĆ Ļ▓ĮļČĆĻ░ÉņŚ╝ņŚÉ ņØśĒĢ£ ņ”ØņāüņØ┤ ņĢäļŗÉ Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ļÉśņŚłņ£╝ļ®░, ņ×ģņøÉ Ēøä ņŗ£Ē¢ēĒĢ£ ņåīļ│ĆĻ▓Ćņé¼ņŚÉņä£ ļ░▒ĒśłĻĄ¼ 5~9/HPF, ņĀüĒśłĻĄ¼ 5~9/HPFĻ░Ć Ļ▓ĆņČ£ļÉśņ¢┤ ĻĖēņä▒ ņŗĀņÜ░ņŗĀņŚ╝ņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłĻ│Ā ļé┤Ļ│╝ļĪ£ ņĀäĻ│╝ļÉśņ¢┤ ĒĢŁņāØņĀ£ ņ╣śļŻīļź╝ ņ¦ĆņåŹĒĢśņśĆļŗż. ļé┤Ļ▓ĮļÅÖļ¦źļźśņŚÉ ļīĆĒĢ£ ņ╣śļŻīļĪ£ ņŗĀĻ▓ĮņÖĖĻ│╝ņŚÉņä£ļŖö ņÜ░ņäĀņĀüņ£╝ļĪ£ ļ╣äņ╣©ņŖĄņĀüņØĖ ņŖżĒģÉĒŖĖ ņŗ£ņłĀ ļ░Å ļÅÖļ¦źļé┤ ĒśłņĀäņĀ£Ļ▒░ņłĀņØä ĒÖśņ×É ļ░Å ļ│┤ĒśĖņ×ÉņŚÉĻ▓ī ĻČīņ£ĀĒĢśņśĆļŗż. ĒĢśņ¦Ćļ¦ī, ņŗ£ņłĀņØś ĒĢ®ļ│æņ”Ø ļ░Å ņ£äĒŚśņä▒ņŚÉ ļīĆĒĢ┤ ņäżļ¬ģņØä ļōżņØĆ ļ│┤ĒśĖņ×ÉļōżņØĆ Ļ│ĀļĀ╣ņØĖ ņĀÉņØä Ļ│ĀļĀżĒĢśņŚ¼ ņČöĻ░ĆņĀüņØĖ ņ╣śļŻīļź╝ Ļ▒░ņĀłĒĢśņśĆĻ│Ā, ņØ┤ņŚÉ ĒĢŁĒśłņĀäņĀ£ļź╝ ĒżĒĢ©ĒĢ£ ļ│┤ņĪ┤ņĀü ņ╣śļŻīļź╝ ĒĢśļ®░ Ļ▓ĮĻ│╝Ļ┤Ćņ░░ ĒĢśĻĖ░ļĪ£ ĒĢśņśĆņ£╝ļ®░, Ēśäņ×¼Ļ╣īņ¦Ć ņ¦äļŗ© Ēøä 20Ļ░£ņøö ļÅÖņĢł ĒĢ®ļ│æņ”Ø ņŚåņØ┤ ņÖĖļל ņČöņĀü Ļ┤Ćņ░░ ņżæņØ┤ļŗż.
Ļ│Ā ņ░░
ļé┤Ļ▓ĮļÅÖļ¦źļźś[internal carotid artery(ICA) aneurysm]ļŖö ļ░£ņāØĒĢśļŖö ĒĢ┤ļČĆĒĢÖņĀü ņ£äņ╣śņŚÉ ļö░ļØ╝ ļæÉĻ░£ļé┤(intracranial)ņÖĆ ļæÉĻ░£ņÖĖ(extracranial)ļĪ£ ļéśļłī ņłś ņ׳ņ£╝ļ®░, ļæÉĻ░£ļé┤ ļé┤Ļ▓ĮļÅÖļ¦źļźśļŖö ņŚ¼ļ¤¼ļČäņ¦ĆņŚÉ Ļ▒Ėņ│É ļ░£ņāØĒĢśļŖö ļ░®ņČöĒśĢ(fusiform)Ļ│╝ ļ░£ņāØĒĢśļŖö ļČäņ¦ĆņŚÉ ļö░ļØ╝ ļé┤Ļ▓Į-ņĢł ļÅÖļ¦ź(ICA-ophthalmic artery junction), ļé┤Ļ▓Į-ĒøäĻĄÉĒåĄ ļÅÖļ¦ź(ICA-posterior communicating artery junction), ļé┤Ļ▓Į-ņĀäļ¦źļØĮ ļÅÖļ¦ź(ICA-anterior choroidal artery junction), ļé┤Ļ▓ĮļÅÖļ¦ź ļČäĻĖ░(ICA bifurcation) ļÅÖļ¦źļźśļĪ£ ļéśļēśņ¢┤ņ¦äļŗż[6]. ļæÉĻ░£ļé┤ļČĆņÖĆ ņÖĖļČĆņØś ĒśłĻ┤ĆņØĆ ņĪ░ņ¦üĒĢÖņĀü ĻĄ¼ņĪ░Ļ░Ć ļŗ¼ļØ╝ ļŗżļźĖ ļ│æļ”¼ņāØĒā£ĒĢÖņĀü ņÜöņØĖņ£╝ļĪ£ ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśļ®░[7], ļæÉĻ░£ļé┤ņŚÉ ļ░£ņāØĒĢśļŖö ļćīļÅÖļ¦źļźś(cerebral aneurysm) ņżæ ļé┤Ļ▓ĮļÅÖļ¦źņØĆ Ļ░Ćņן ĒØöĒĢśĻ▓ī ļ░£ņāØĒĢśļŖö ņ£äņ╣śļĪ£ ņĢīļĀżņĀĖ ņ׳Ļ│Ā, ļæÉĻ░£ņÖĖ ļé┤Ļ▓ĮļÅÖļ¦źļźśļŖö ļ╣äĻĄÉņĀü ĒØöņ╣ś ņĢŖņØĆ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[8].
ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźśļŖö ņĀäņ▓┤ ļÅÖļ¦źļźśņØś ņĢĮ 0.4~1% ņĀĢļÅäļ¦īņØä ņ░©ņ¦ĆĒĢśļŖö ļ╣äĻĄÉņĀü ļō£ļ¼Ė ņ¦łĒÖśņ£╝ļĪ£[1], ņ┤ØĻ▓ĮļÅÖļ¦ź(common carotid artery), ņÖĖĻ▓ĮļÅÖļ¦ź(external carotid artery), ļé┤Ļ▓ĮļÅÖļ¦źņŚÉņä£ ļ¬©ļæÉ ļ░£ņāØĒĢĀ ņłś ņ׳ņ£╝ļéś, Ļ░Ćņן ĒØöĒ׳ ļ░£ņāØĒĢśļŖö ņ£äņ╣śļŖö Ļ▓ĮļÅÖļ¦ź ļČäĻĖ░(carotid artery bifurcation)ņØ┤ļ®░[9] ņÖĖĻ▓ĮļÅÖļ¦źņŚÉ ļ░£ņāØĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć Ļ░Ćņן ļō£ļ¼╝ļŗż[10]. ņ┤ØĻ▓ĮļÅÖļ¦źņØś ņ¦üĻ▓ĮņØ┤ 150% ņØ┤ņāüņØ╝ ļĢī ņ¦äļŗ©ĒĢĀ ņłś ņ׳ņ£╝ļ®░, ļé┤Ļ▓ĮļÅÖļ¦źņØś Ļ▓ĮņÜ░ļŖö ņ¦üĻ▓ĮņØś 200% ņØ┤ņāü ĒīĮņ░ĮļÉśņ¢┤ ņ׳Ļ▒░ļéś ļŗ©ļ®┤ņĀüņØ┤ ļÅÖņĖĪ ņĀĢņāü ļÅÖļ¦źņØś 120% ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ņŚÉļÅä ļÅÖļ¦źļźśļĪ£ Ļ░äņŻ╝ļÉ£ļŗż[11]. Ļ░ÉņŚ╝, ņÖĖņāü, ļÅÖļ¦źĒśłĻ┤ĆņØś ņäĀņ▓£ņä▒ ļśÉļŖö ļ░£ļŗ¼ņä▒ Ļ▓░ĒĢ©, ņä¼ņ£ĀĻĘ╝ņØ┤ĒśĢņä▒ ļō▒ņØś ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć ņØ┤ņ£ĀļĪ£ ļ░£ņāØĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ņĄ£ĻĘ╝ņŚÉļŖö ļÅÖļ¦źĻ▓ĮĒÖöņ”Ø ļ░Å Ļ▓ĮļÅÖļ¦ź ļé┤ļ¦ē ņĀłņĀ£ņłĀņØ┤ļéś ĒśłĻ┤Ć ņĪ░ņśüņłĀĻ│╝ Ļ░ÖņØĆ ņŗ£ņłĀ Ēøä ļ░£ņāØĒĢ£ Ļ░ĆļÅÖļ¦źļźś ļō▒ņØ┤ ņŻ╝ļÉ£ ņøÉņØĖņ£╝ļĪ£ Ļ╝ĮĒ׳Ļ│Ā ņ׳ļŗż[2,12]. ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźśļŖö ļ¼┤ņ”Øņāüņ£╝ļĪ£ ļ░£Ļ▓¼ļÉśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ņ¦Ćļ¦ī, ļćīĒŚłĒśłņØ┤ļéś ļćīĻ▓Įņāē ļō▒ņØś ņŗĀĻ▓ĮĒĢÖņĀü ĒĢ®ļ│æņ”Ø, ĻĄŁņåī ņĢĢļ░ĢņŚÉ ņØśĒĢ£ ņŗĀĻ▓ĮĒĢÖņĀü ņ”ØņäĖ, ņČ£ĒśłļĪ£ ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äņ£╝ļ®░, ņä▒ņØĖĻ│╝ ņåīņĢäņŚÉņä£ Ļ│ĄĒåĄņĀüņ£╝ļĪ£ ļ░ĢļÅÖņä▒ Ļ▓ĮļČĆ ņóģĻ┤┤Ļ░Ć Ļ░Ćņן ĒØöĒĢ£ ņ”ØņāüņØ┤ļŗż[3,13].
ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźśļŖö ļ░£ņāØ ņ£äņ╣śņŚÉ ļö░ļØ╝ ņ”ØņāüņØ┤ ļŗżļź┤Ļ▓ī ļéśĒāĆļéĀ ņłś ņ׳ļŖöļŹ░, Ļ▓ĮļČĆ ņóģĻ┤┤ ņŚåņØ┤ ĻĄ¼ņØĖļæÉļé┤ ņóģņ░ĮņØś ĒśĢĒā£ļ¦īņ£╝ļĪ£ ļéśĒāĆļéśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ļé┤Ļ▓ĮļÅÖļ¦źņØś ņāüĻ▓ĮļČĆ ļČäņĀł(high cervical segment)ņŚÉ ļ░£ņāØĒĢ£ ļÅÖļ¦źļźśĻ░Ć ĒÄĖļÅäņÖĆņ¬Įņ£╝ļĪ£ļ¦ī ĒÖĢņןļÉśņ¢┤ņĢ╝ ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ļ¤¼ĒĢ£ Ļ▓ĮņÜ░ļŖö ļ¦żņÜ░ ļō£ļ¼╝ļŗż[14,15]. ļö░ļØ╝ņä£, ļæÉĻ░£ņÖĖ ļé┤Ļ▓ĮļÅÖļ¦źļźśĻ░Ć ĻĄ¼Ļ░Ģļé┤ņØś ņóģĻ┤┤ ĒśĢĒā£ļ¦īņ£╝ļĪ£ ļ░£ĒśäļÉĀ Ļ▓ĮņÜ░ ņÜ░ņäĀņĀüņ£╝ļĪ£ ļé┤Ļ▓ĮļÅÖļ¦źļźśļź╝ ņØśņŗ¼ĒĢśĻĖ░ļŖö ņēĮņ¦Ć ņĢŖņ£╝ļ®░, ĒŖ╣Ē׳ ļ│Ė ņ”ØļĪĆņÖĆ Ļ░ÖņØ┤ Ļ│ĀņŚ┤ ļ░Å ņØĖĒøäĒåĄ ļō▒ņØś ļŗżļźĖ ņ”ØņāüĻ│╝ ļÅÖļ░śļÉĀ Ļ▓ĮņÜ░ ņØ┤ĒĢÖņĀü Ļ▓Ćņé¼ļ¦īņ£╝ļĪ£ Ļ░Éļ│äĒĢśĻĖ░Ļ░Ć ņēĮņ¦Ć ņĢŖļŗż. ļśÉĒĢ£ ļ░śļ│ĄņĀüņØĖ ĒÄĖļÅäņŚ╝ņØ┤ļéś ĒÄĖļÅäņŻ╝ņ£ä ļåŹņ¢æņØś ĒĢ®ļ│æņ”Øņ£╝ļĪ£ ĒśłĻ┤ĆņŚ╝ņØ┤ ļ░£ņāØĒĢśņŚ¼ ĒśłĻ┤ĆņØś ļ▓ĮņØ┤ ņĢĮĒĢ┤ņ¦ĆĻ▒░ļéś ļ»Ėļ×Ć(erosion)ņ£╝ļĪ£ ņØĖĒĢ┤ ņČ£ĒśłņØ┤ļéś ļÅÖļ¦źļźśĻ░Ć ļ░£ņāØĒĢĀ ņłś ņ׳ņ¢┤, ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æĻ│╝ ļÅÖļ¦źļźśĻ░Ć ĒĢ©Ļ╗ś ļ░£Ļ▓¼ļÉĀ ņłśļÅä ņ׳ļŗż. 1974ļģä ĒÄĖļÅäņŻ╝ņ£ä ļåŹņ¢æĻ│╝ ļé┤Ļ▓ĮļÅÖļ¦źļźśĻ░Ć ĒĢ©Ļ╗ś ļ░£Ļ▓¼ļÉ£ ņ”ØļĪĆĻ░Ć ļ│┤Ļ│ĀļÉśĻĖ░ļÅä ĒĢśņśĆļŗż[16].
ņĄ£ĻĘ╝ 20ļģä ļÅÖņĢł ļæÉĻ░£ņÖĖ ļé┤Ļ▓ĮļÅÖļ¦źļźśĻ░Ć ĻĄ¼ņØĖļæÉ ņóģĻ┤┤ļĪ£ ļ░£Ļ▓¼ļÉ£ ļ¼ĖĒŚī ļ│┤Ļ│ĀļŖö ļ¦Äņ¦Ć ņĢŖņØĆļŹ░, ļīĆļČĆļČä ņŚ╝ņ”ØņåīĻ▓¼ņØĆ ļÅÖļ░śļÉśņ¦Ć ņĢŖĻ│Ā ņŚ░ĒĢśĻ│żļ×ĆņØä ņŻ╝ņ”Øņāüņ£╝ļĪ£ ĒĢśņśĆĻ│Ā ĒÄĖņĖĪļ¦łļ╣ä(hemiplegia)ļéś ĒśĖļäłņ”ØĒøäĻĄ░ņØ┤ ļÅÖļ░śļÉśĻĖ░ļÅä ĒĢśņŚ¼ ļÅäĒöīļ¤¼ ņ┤łņØīĒīī, ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü, ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņØä ĒåĄĒĢśņŚ¼ ļÅÖļ¦źļźśļź╝ ņ¦äļŗ©ĒĢśņśĆņ£╝ļ®░ ņŻ╝ļĪ£ ņłśņłĀņĀü ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż(Table 1)[3,4,15,17-20]. ņØ┤ ņżæņŚÉņä£ ļ░£ņŚ┤ņØ┤ļéś ņŚ╝ņ”ØņåīĻ▓¼ņØ┤ ļÅÖļ░śļÉśņ¢┤ ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņ£╝ļĪ£ ņśżņØĖļÉ£ Ļ▓ĮņÜ░ļŖö 2ņśłĻ░Ć ņ׳ņŚłĻ│Ā, 4ņäĖ ņåīņĢäĒÖśņ×ÉņŚÉņä£ Ļ▓ĮļČĆ ņóģļ¼╝Ļ│╝ ĒĢ©Ļ╗ś ĒÄĖļÅäņŻ╝ņ£ä ņóģņ░Į ļ░Å ļ░£ņŚ┤ņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņŚ¼ ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņ£╝ļĪ£ ņśżņØĖĒĢ£ ņ”ØļĪĆ[5]Ļ░Ć ļ│┤Ļ│ĀļÉśņŚłņ£╝ļéś, ĻĄŁļé┤ņŚÉņä£ļŖö ņĢäņ¦üĻ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ ļ░öĻ░Ć ņŚåņŚłļŗż.
ļé┤Ļ▓ĮļÅÖļ¦źļźśņŚÉ ļīĆĒĢ┤ņä£ļŖö ņłśņłĀņĀü ņ╣śļŻīĻ░Ć ĻČīĻ│ĀļÉśļ®░, ņłśņłĀņØ┤ ņĢäļŗī ļ│┤ņĪ┤ņĀü ņ╣śļŻīņØś Ļ▓ĮņÜ░ ņāēņĀäņ”Ø ļō▒ņØś ļ░£ņāØ ņ£äĒŚśņä▒ņØ┤ ļåÆņĢä ņØ╝ļČĆ ĒÖśņ×ÉĻĄ░ņØä ņĀ£ņÖĖĒĢśĻ│ĀļŖö ĻČīĻ│ĀļÉśņ¦Ć ņĢŖļŖöļŗż. ņłśņłĀņĀü ņ╣śļŻīļĪ£ļŖö ļÅÖļ¦źļźś ņĀłņĀ£ņłĀ ļ░Å ņ¢æņĖĪ ļŗ©ļŗ©ļ¼ĖĒĢ®ņłĀ(resection with end-to-end anastomosis), ļÅÖļ¦źļźś Ļ▓░ņ░░(ligation), ļæÉĻ░£ļé┤ņÖĖņÜ░ĒÜīļĪ£ņĪ░ņä▒ņłĀ(extracranial intracranial bypass) ļō▒ņØś ļ░®ļ▓ĢļōżņØ┤ ņŗ£ļÅäļÉśĻ│Ā ņ׳ļŗż[12]. ļŗżļ¦ī, ņØ┤ņÖĆ Ļ░ÖņØĆ Ļ┤ĆĒśłņĀü ņłśņłĀ ņ╣śļŻīļŖö ļćīņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ░ÖņØĆ ņŗĀĻ▓ĮĒĢÖņĀü ĒĢ®ļ│æņ”ØņØä ļÅÖļ░śĒĢĀ ņłś ņ׳ņ¢┤, ņØ┤ļź╝ ņżäņØ┤ĻĖ░ņ£äĒĢ£ ļÅÖļ¦źļé┤ ĒśłņĀäņĀ£Ļ▒░ņłĀ, ļÅÖļ¦źļé┤ ņŖżĒģÉĒŖĖ ņéĮņ×ģņłĀ ļō▒ņØś ļ»ĖņäĖ ņ╣©ņŖĄ ņłśņłĀ ļ░®ļ▓ĢļōżņØ┤ ņŗ£ļÅäļÉśĻ│Ā ņ׳ņ£╝ļ®░, ļÅÖļ¦źļé┤ ņŗ£ņłĀņØ┤ Ļ┤ĆĒśłņĀü ņłśņłĀ ņ╣śļŻīņŚÉ ļ╣äĒĢ┤ ļćīņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ░ÖņØĆ ĒĢ®ļ│æņ”ØņØ┤ ņ£ĀņØśĒĢśĻ▓ī ļé«Ļ▓ī ļéśĒāĆļé¼ļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż[21].
ļ│Ė ņ”ØļĪĆņØś ĒÖśņ×ÉļÅä ļÅÖļ¦źļé┤ ņŗ£ņłĀņØä ņÜ░ņäĀņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢśņśĆņ£╝ļéś, ņŗ£ņłĀņØś ĒĢ®ļ│æņ”Ø ļ░Å ņ£äĒŚśņä▒, Ļ│ĀļĀ╣ņØĖ ņĀÉņØä Ļ│ĀļĀżĒĢśņŚ¼, ĒÖśņ×É, ļ│┤ĒśĖņ×ÉņÖĆ ņāüņØś ĒĢś Ļ▓ĮĻ│╝Ļ┤Ćņ░░ ĒĢśĻĖ░ļĪ£ ĒĢśņśĆņ£╝ļ®░, ĒĢŁĒśłņĀäņĀ£ ņ╣śļŻīļź╝ ĒżĒĢ©ĒĢ£ ļ│┤ņĪ┤ņĀü ņ╣śļŻīĒĢśļ®░, ņÖĖļל ņČöņĀü Ļ┤Ćņ░░ ņżæņØ┤ļŗż. ļ│┤ņĪ┤ņĀü ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśļŖö ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźśņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĀĢĒÖĢĒĢ£ ĒĢŁĒśłņĀäņĀ£ņØś ļ│ĄņÜ® ĻĖ░Ļ░äņØ┤ ĻĘ£ņĀĢļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņ£╝ļéś, ņØ╝ļČĆ ņŚ░ĻĄ¼ņŚÉņä£ļŖö 2ņŻ╝ņŚÉņä£ 3Ļ░£ņøö Ļ░äņØś ļ│ĄņÜ®ņØä ņĀ£ņĢłĒĢśĻ│Ā ņ׳ļŗż[22,23]. ļ│Ė ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ Ēśäņ×¼Ļ╣īņ¦Ć ĒŖ╣ļ│äĒĢ£ ĒĢ®ļ│æņ”Ø ņŚåņØ┤ ņāØņĪ┤ ņżæņØ┤ļéś, ņ╣śļŻī ļ░øņ¦Ć ņĢŖņØĆ ļæÉĻ░£ņÖĖ Ļ▓ĮļÅÖļ¦źļźś ĒÖśņ×ÉņØś Ļ▓ĮņÜ░, ļ░śļō£ņŗ£ 71%ņŚÉņä£ ļÅÖļ¦źļźś ĒīīņŚ┤ļĪ£ ņØĖĒĢ£ ņé¼ļ¦ØņØś ņ£äĒŚśņä▒, 50%ņŚÉņä£ ļćīņĪĖņżæņØś ļ░£ņāØ ņ£äĒŚśņä▒ ļō▒ ņ╣śļ¬ģņĀüņØĖ ĒĢ®ļ│æņ”ØņØ┤ ņ£Āļ░£ļÉĀ ņłś ņ׳ļŗżļŖö ņĀÉ[12], ņČöĒøä ļÅÖļ¦źļźśņØś ĒÖĢņןņ£╝ļĪ£ ņØĖĒĢ£ ĻĖ░ļÅä ņĢĢļ░Ģ ļ░Å ĒśĖĒØĪĻ│żļ×Ć, ļ»ĖņŻ╝ņŗĀĻ▓Į ļō▒ņØś ļćīņŗĀĻ▓Į ņĢĢļ░Ģņ£╝ļĪ£ ņØĖĒĢ£ ļ¬®ņåīļ”¼ ļ│ĆĒÖö, ņåīĒÖöĻĖ░Ļ│ä ņĢĢļ░Ģņ£╝ļĪ£ ņØĖĒĢ£ ņŚ░ĒĢśĻ│żļ×Ć ļō▒ņØś ņ”Øņāü ļ░£ņāØ Ļ░ĆļŖźņä▒[20]ņŚÉ ļīĆĒĢ┤ ņČ®ļČäĒ׳ Ļ│Āņ¦ĆĒĢ┤ņĢ╝ ĒĢ£ļŗż.
ņØ╝ļ░śņĀüņ£╝ļĪ£ ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņØ┤ ņØśņŗ¼ļÉĀ Ļ▓ĮņÜ░ ļČĆņóģ ļČĆņ£äņŚÉ ļīĆĒĢ£ ņ▓£ņ×ÉĒØĪņØĖ ļō▒ņ£╝ļĪ£ ļåŹņ¢æņØä ĒÖĢņØĖĒĢśņŚ¼ ņ¦äļŗ©ĒĢśĻ▒░ļéś, ņĄ£ĻĘ╝ņŚÉļŖö ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü Ēś╣ņØĆ ņ┤łņØīĒīīļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ļåŹņ¢æņØś ņŚ¼ļČĆļź╝ ĒÖĢņØĖĒĢ£ ļÆż ņ▓£ņ×ÉĒØĪņØĖ Ēś╣ņØĆ ņĀłĻ░£ļ░░ļåŹ ļō▒ņØś ņŗ£ņłĀņØä ņŗ£Ē¢ēĒĢśĻ▓ī ļÉ£ļŗż[24]. ĒĢśņ¦Ćļ¦ī ļ│Ė ņ”ØļĪĆņŚÉņä£ņÖĆ Ļ░ÖņØ┤ ļ░£ņŚ┤ņØ┤ļéś ņØĖĒøäĒåĄ ļō▒ņØś ņŚ╝ņ”ØņåīĻ▓¼ņØ┤ ļÅÖļ░śļÉ£ ĻĄ¼Ļ░Ģļé┤ ņóģņ░ĮņØś Ļ▓ĮņÜ░ņŚÉļŖö ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņ£╝ļĪ£ ņśżņØĖĒĢĀ ņłś ņ׳Ļ│Ā, ņØ┤ņŚÉ ļīĆĒĢ┤ņä£ ņ┤łņØīĒīī ļśÉļŖö Ļ▓ĮļČĆ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü ļō▒ņØś ņśüņāüĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖĻ│Ā ņ×äņāüĒĢÖņĀü ņ¦äļŗ©ļ¦īņ£╝ļĪ£ ņ×äņØśļĪ£(blind) ņ▓£ņ×ÉĒØĪņØĖ, Ēś╣ņØĆ ņĀłĻ░£ļ░░ļåŹņØä ņŗ£Ē¢ēĒ¢łņØä Ļ▓ĮņÜ░, Ļ▓ĮļÅÖļ¦ź ĒīīņŚ┤ ļ░Å ĻĘĖļĪ£ ņØĖĒĢ£ Ļ│╝ļŗżņČ£Ēśł, ļćīņĪĖņżæ ļō▒ņØś ņ╣śļ¬ģņĀüņØĖ ĒĢ®ļ│æņ”ØņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗż. ņØ┤ņĀä ļ¼ĖĒŚīņŚÉņä£ļÅä ĒÄĖļÅäņŻ╝ņ£äļåŹņ¢æņ£╝ļĪ£ ņśżņØĖĒĢśņŚ¼ ņ▓£ņ×É Ēøä ļÅÖļ¦ź ņČ£ĒśłņØ┤ ļ░£ņāØĒĢśņŚ¼ ņ”ēĻ░ü ņżæļŗ©ĒĢśņśĆņ£╝ļéś 6 cmņ£╝ļĪ£ Ēü¼ĻĖ░Ļ░Ć ĻĖēĻ▓®Ē׳ ņ”ØĻ░ĆĒĢśņŚ¼ ņŚ░ĒĢśņןņĢĀ ļ░Å ņŗ¼Ļ░üĒĢ£ ņśüņ¢æņŗżņĪ░Ļ░Ć ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░[19]ņÖĆ ņĀłĻ░£ Ēøä ļīĆļ¤ē ņČ£ĒśłņØ┤ ļ░£ņāØĒĢśņśĆļŹś Ļ▓ĮņÜ░[12]Ļ░Ć ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░, ļæÉ ĒÖśņ×É ļ¬©ļæÉ ņĀüĻĘ╣ņĀüņØĖ ņłśņłĀņĀü ņ╣śļŻīļź╝ ļ░øņØĆ ļÆż ņāØņĪ┤ĒĢĀ ņłś ņ׳ņŚłņ¦Ćļ¦ī ļīĆļ¤ē ņČ£ĒśłņØś ņ£äĒŚśņä▒ņØä ņĢī ņłś ņ׳ņŚłļŗż. ņĀĆņ×ÉļŖö ļ│Ė ņ”ØļĪĆļź╝ ĒåĄĒĢ┤ ĒÄĖļÅäņŻ╝ņ£ä ņóģņ░ĮņØä ļ│┤ņØ┤ļŖö ĒÖśņ×ÉĻ░Ć ļé┤ņøÉĒĢĀ Ļ▓ĮņÜ░, ņŚ╝ņ”Ø ņåīĻ▓¼ņØ┤ ļÅÖļ░śļÉśņ¢┤ Ļ▓ĮļČĆ Ļ░ÉņŚ╝ ļ░Å ļåŹņ¢æ ĒśĢņä▒ņØ┤ ņØśņŗ¼ļÉśļŹöļØ╝ļÅä, ņ▓£ņ×ÉĒØĪņØĖ ļ░Å ņĀłĻ░£ļ░░ļåŹ ļō▒ņØś ņŗ£ņłĀ ņĀä ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü ļśÉļŖö ņ┤łņØīĒīī ļō▒ņØś ņśüņāüĒĢÖņĀü Ļ▓Ćņé¼Ļ░Ć ĒĢäņÜöĒĢśļ®░, ļé┤Ļ▓ĮļÅÖļ¦źļźśļÅä Ļ░Éļ│äņ¦łĒÖśņ£╝ļĪ£ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗżĻ│Ā ņāØĻ░üļÉśņ¢┤ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśļŖö ļ░öņØ┤ļŗż.