상악동 진균구의 범위에 따른 수술 후 결과 차이
Abstract
Background and Objectives
Fungus ball is the most common type of fungal sinusitis commonly associated with good prognosis. However, postoperative results depending on the extent of the lesion has not been investigated. This study aimed to identify differences in postoperative results depending on the location and extent of the fungus ball.
Subjects and Method
Medical records of 165 patients who underwent endoscopic sinus surgery and who were diagnosed with fungus balls by biopsy from 2010 to 2019 were retrospectively reviewed. Patients were classified into four grades according to the location and extent of the fungus ball based on their endoscopic and CT findings. Poor outcome is defined as any pathologic signs such as nasal secretion, granulation, and polyps or narrowing of the natural ostium observed postoperatively according to Kennedy’s criteria, whereas good outcome is defined as absence of pathologic signs.
Results
A total of 23 patients were Grade 1, 38 Grade 2, 67 Grade 3, and 37 Grade 4. Grades 1 and 2 were mostly asymptomatic. However, as the location of the fungus ball became closer to the natural ostium, patients complained postnasal drip and purulent discharge. Grades 3 and 4, who have much severe and more extensive lesions than those of Grades 1 and 2, had poor outcome (p=0.007) and took longer time to completely recover (p<0.001).
Conclusion
Wound healing was delayed and poor when the fungus ball was located closer to the natural ostium of the maxillary sinus. Therefore, preoperative consultation using endoscopic and CT findings could be useful for predicting their postoperative results.
Key words: Fungus ball ㆍ Maxillary sinus ㆍ Wound healing
서 론
진균성 부비동염은 일반적으로 침습성과 비침습성으로 나눌 수 있는데, 이 중 진균구는 비침습형 진균성 부비동염 중 가장 많은 비율을 차지하는 질환이다. 진균구는 균사가 점막 침범없이 비부비강 점막 밖에 자라는 것이 특징인 질환으로 최근 진단 장비의 발달과 더불어 면역 저하를 야기하는 질환의 증가 등의 이유로 유병률이 늘어나는 추세이다[ 1, 2]. 수술 후 경과에 대해서 한 연구에서는 3.2%의 환자만이 재발하였다고 보고하였으나[ 3], 실제 임상에서는 환자들마다 진균구의 위치 및 병변의 범위에 따라 임상 양상이 다양하며, 술후 예기치 않은 상악동 개방부의 협착이나 페쇄 등 결과가 좋지 않은 환자도 경험하기도 한다. 이에 저자들은 상악동에 국한되어 발생하는 진균구 환자에서 수술 전 병변의 위치와 범위가 수술 후 회복 과정 및 결과에 영향을 미치는지 알아보고자 하였다.
대상 및 방법
대 상
2010년 1월~2019년 4월까지 부비동 내시경 수술을 받은 환자 중 조직검사 결과가 진균구로 진단된 환자를 대상으로 하였다. 수술 후 3개월까지 외래 추적 관찰이 시행된 165명의 환자들을 대상으로 의무기록을 후향적 분석을 시행하였다. 본 연구에 포함된 환자의 수술 및 수술 후 치료는 2인의 숙련된 전문의(YJ Chung, JH Mo)에 의해 시행되었다.
퇴원 시 대부분 환자들에게 경구 항생제 및 비강 스테로이드 스프레이를 1주일간 처방하였으며, 이후 병적인 증상이나 증거가 없으면 처방하지 않았다. 수술 후 외래 추적 관찰은 수술 후 1주일째, 3주일째, 이후는 한 달 간격으로 시행하였으나 비분비물, 부종, 비용종 또는 상악동의 자연공이 좁아진 경우와 같이 병적 증거가 있는 경우에는 경구 항생제나 비강 내 스테로이드 스프레이를 포함한 약물 처방 또는 touch up procedure 후 2주 이내 진료를 시행하였다.
본 연구는 본원의 기관생명윤리위원회 심의를 통과하였다(DKUH-2020-02-023).
창상 치유의 기준
수술을 받은 환자들은 추적 관찰 때마다 비강 내시경 소견을 촬영하였다. 이를 토대로 수술 후 3개월째 시행한 비강 내시경 소견을 분석하였고, Kennedy [ 4]가 제시한 기준에 근거하여 비분비물, 부종, 비용종과 같은 병적 증거가 하나라도 없으며 상악동의 자연공이 잘 유지가 되는 경우에는 ‘결과가 좋은 군,’ 이와 반대로 병적 증거가 하나라도 있는 경우는 ‘결과가 나쁜 군’으로 분류하였다( Fig. 1).
진균구 위치의 분류
수술 전 시행한 비강 내시경 소견과 전산화단층촬영[(ostiomeatal unit, OMU)-CT]를 이용하여 분석하였다. 진균구의 위치 및 염증의 범위에 따라 총 4단계로 분류하였으며 1단계는 내시경 상 비강 내 특이 소견이 관찰되지 않고 CT에서는 상악동 혼탁이 저부에만 존재할 때, 2단계는 내시경에서 비강 내 농성 분비물이 보이고 CT에서 상악동 중간 위치 정도까지 혼탁이 관찰될 때, 3단계는 내시경에서 비강 내 농성 분비물이 보이고 CT에서 혼탁이 자연공까지 침범하였을 때, 그리고 4단계는 내시경상 농성 분비물이 보이고 CT상 혼탁이 개구비도단위(OMU)까지 보이는 경우로 분류하였다( Fig. 2).
통계분석
통계분석은 SPSS version 25(IBM Corp., Armonk, NY, USA)을 이용하여 진균구 위치와 인구통계학, 치아 상태, 창상 치유 및 예후와의 상관성을 비교하기 위해 chi-square test 및 one-way analysis of variance test를 이용하였고, 각 Grade 간 회복 기간을 비교하기 위해 Kaplan-Meier 생존곡선을 이용하였다.
결 과
165명 중 남성이 55명(33%), 여성이 110명(67%)이었으며, 평균 연령은 60.9±11.8세(28~85세)였다. 일측성인 경우가 158명(95.8%)로 대부분이었고, 기저질환으로 당뇨가 있는 환자는 29명(17.6%), 천식이 있는 환자는 3명(1.8%)의 비율을 보였다. 전형적인 알레르기 비염 증상(코막힘, 수양성 비루, 재채기, 가려움증)을 호소하며 피부반응 검사나 multiple allergen simultaneous test(MAST), UNICAP 검사에서 양성반응을 보인 알레르기 비염 환자들의 비율은 26명(15.8%)이였다( Table 1). Grade 1은 23명(14%), Grade 2는 38명(23.8%), Grade 3은 67명(40.6%), 가장 심한 Grade 4는 37명(22.4%)으로, Grade 3이 가장 많은 비율을 보였다. 흡연과의 연관성은 Grade 간 차이가 관찰되었으나( p=0.007), 다른 인자들과의 상관성은 보이지 않았다( Table 2). 무증상(우연히 발견된 경우)이 가장 많았고(n=30, 18%), 다음으로는 코막힘(n=27, 16%)이 가장 많았다. Grade 1과 2 환자에서는 무증상이 가장 많았으나, Grade 3과 4 환자에서는 무증상인 경우는 낮았으며 화농성 비루나 후비루 등 증상이 있는 경우가 대부분이었다( Table 3). 진균구와 연관성이 있는 치아 상태를 확인하고자 환자들의 병력 및 전산화단층촬영을 통하여 평가하였고, 정상, 치아 보철물, 임플란트, 치성농양으로 4가지로 분류하였다. 모든 환자에서 치아 문제가 있는 환자들의 비율이 비교적 높은 경향을 보였으며, Grade 1을 제외한 환자들에게서 과반수 이상이 치아 문제가 있는 것으로 확인되었으나 통계적인 연관성은 보이지 않았다( Table 4). 창상 치유는 병변이 진행될수록, 즉 진균구의 위치 및 병변의 범위가 상악동의 자연공으로 진행될수록, 창상 치유가 좋지 않았으며 통계적으로도 유의한 결과를 보였다( p=0.005). 외래 추적 관찰 시 비용종 및 과립, 자연공이 좁아진 경우가 확인된 환자들에게서 touch-up을 시행하였는데 Grade 1과 2 환자에서는 각각 1명(4.34%, 2.63%)에게 시행하였고, Grade 3와 4 환자에서는 각각 4명(5.97%, 10.8%)으로 확인되었다. 통계적인 연관성을 보이지 않았지만, Grade 1과 2 환자들보다 Grade 3와 4의 touch up 비율이 높은 경향을 보였다( p=0.251) ( Table 5). 술후 회복 기간의 경우 Grade 1 환자들이 10.5±2.8주로 가장 짧았다.
Grade 2는 10.9±3.6주, Grade 3는 15.1±6.7주였으며 Grade 4 환자들이 16.3±6.8주로 가장 길었다. 병변이 자연공에 가까이 위치하고 병변이 심할수록, 회복 기간의 기간이 통계적으로 유의하게 길어지는 양상을 보였다( p=0.001)( Table 6, Fig. 3).
고 찰
진균구의 발생기전은 아직 명확히 밝혀지지 않았으나 부비동의 염증으로 인해 개구비도단위(OMU)가 폐쇄되고 이로 인해 부비동의 자연공이 막혀 진균 성장에 좋은 환경이 만들어져 발생한다는 가설이 있다[ 1]. 진균구는 상악동에 주로 발생하며[ 5], 수술적 방법으로 이를 제거하면 대부분 예후가 좋은 것으로 알려져 있다[ 6]. Nicoli 등[ 2]의 보고에 따르면 135명의 상악동 진균구 환자들에게서 부비동 내시경 수술을 시행한 결과, 2명(1.48%)의 환자만이 진균구의 재발 소견으로 인해 상악동 개방 부위의 협착이 발생하였다고 보고하였고 추가적인 수술 이후에는 재발없이 잘 회복되었다고 보고하였다. Dufour 등7)은 173명의 진균구 환자들에게서 술 후 단 1명(0.57%)의 재발을 보고하였으며, 그 외에도 대부분 재발의 비율을 0~10%로 좋은 예후에 대해 보고하였다[ 2, 5, 8, 9]. 본 연구에서는 진균구가 재발하여 재수술을 한 경우는 없었으나, 수술 부위인 상악동 자연공 개방부의 협착 등의 소견으로 간단히 touch-up 시술을 10명(6.06%)의 환자에게 시행하였다. 진균구가 치과용 충전물질들에 의해 이차적으로 발생한다는 연구들이 보고되었는데[ 7, 10- 12], 본 연구에서도 각 군 간 통계적 차이 없이 치아 문제가 있는 환자들의 비율이 높은 경향을 보였지만, 대조군과의 비교를 하지 않아 선행 연구 결과를 확인할 수는 없었다. 하지만, 기존 연구 결과 67.3%에서 관찰되어 간접적으로는 이에 유사한 결과를 도출하였다[ 13]. 한편 진균구의 증상은 비특이적이면서 다양하기 때문에 다른 부비동염과 진단이 어려울 때도 있다[ 14]. 진균구가 침범된 부비동에 따라 증상이 다양한데 상악동에 침범된 경우 안면통이나 화농성 비루, 후비루, 코막힘이 대부분이고 무증상인 경우도 있다[ 9, 15]. 많은 연구들이 진균구가 침범된 부비동에 따라 증상을 나누었으나 본 연구에서는 상악동 내에서 진균구의 위치에 따라 증상을 분석하였다. 진균구가 상악동의 자연공과 가까울수록 호소하는 증상이 많았고, 멀수록 증상이 없었다. 흥미로운 점은 Grade 4 환자들이 가장 많이 호소한 증상은 코막힘 이였는데, 이는 비강 기류를 가장 많이 통과하는 중비도가[ 16] 진균구의 침범으로 인해 막혀 발생한 현상으로 보인다. 대부분의 연구가 진균구의 재발 여부에 따라서 예후를 결정하였고, 수술 후 창상 치유나 부비동 개방 부위의 협착 유무 등 회복 과정 면에서 결과를 분석한 연구는 아직까지 보고된 바가 없다. 저자들은 수술 후 창상 부위 회복이 오래 걸리거나 부비동의 자연공이 좁아지는 경우 등 예후가 좋지 않은 환자들을 종종 경험하여 본 연구를 진행한 결과에서 진균구의 위치와 병변의 범위가 연관이 있음을 확인하였다. 즉 진균구가 상악동 저부에만 존재할 경우 비교적 병변이 덜 진행된 것으로 보이며, 상악동의 염증성 병변이 커질수록 진균구가 상악동의 자연공 쪽으로 밀려 더 넓은 상악동 병변이 발생하여 술 후 창상 치유가 지연되고 상악동의 자연공이 좁아질 확률이 높아질 것으로 보인다. 상악동 진균성 부비동염의 진행이 1단계의 병변이 심해져 2, 3, 4단계의 순서로 진행되는 일련의 과정으로 추측해볼 수 있으나, 본 연구는 횡단연구이기 때문에 추가적인 연구가 필요할 것으로 보인다.
결론적으로 진균구가 상악동의 자연공에 가까울수록 창상 치유 기간이 길고 상악동의 자연공이 협착될 가능성이 높으며, touch-up과 같은 추가적인 처치가 필요한 경우가 호발할 수 있으므로 이러한 환자들에게서 수술 전 충분한 설명과 병변이 심한 경우에는 상악동 개방확장술(mega-antrostomy)같은 술식이 도움이 될 것으로 생각된다. 이 연구 결과를 토대로 수술 전 내시경 소견과 전산화단층촬영 소견을 이용해 종합적으로 평가한다면 상악동 진균구 환자들의 수술 후 창상 치유 및 예후, 수술 시와 수술 후 추가적인 조치를 예측하는데 있어 도움이 될 것으로 생각된다.
ACKNOWLEDGMENTS
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (2019 R1F1A1060589).
Notes
Author Contribution
Conceptualization: Yonug-Jun Chung, Ji-Hun Mo, Ki-Yong Choi, Kwang-Hyun Byun, Jung-Hyun Ahn. Data curation: Yeo-Rim Ju, Ki-Yong Choi, Kwang-Hyun Byun, Jung-Hyun Ahn. Formal analysis: Yonug-Jun Chung, Yeo-Rim Ju, Ji-Hun Mo, Ki-Yong Choi. Funding acquisition: Young-Jun Chung, Yeo-Rim Ju, Ki-Yong Choi. Investigation: Ki-Yong Choi, Kwang-Hyun Byun. Methodology: Yonug-Jun Chung, Yeo-Rim Ju, Ji-Hun Mo, Jung-Hyun Ahn. Project administration: Yonug-Jun Chung, Yeo-Rim Ju, Kwang-Hyun Byun. Supervision: Yonug-Jun Chung, Ji-Hun Mo, Ki-Yong Choi. Visualization: Yonug-Jun Chung, Ji-Hun Mo. Writing—original draft: Yeo-Rim Ju. Writing—review & editing: all authors.
Fig. 1.
A good and poor post operational outcome. Good outcome is characterized by a blood clot and packing material around the MMA site (A), and the MMA site is well maintained without stenosis, granulation, and edema at 1 month (B) and 3 months (C) postoperatively. Poor outcome status shows similar to (A) at 1 week postoperatively (D). However, the natural ostium of the maxillary sinus is narrowed and poorly maintained after 1 month (E) to 3 months (F) postoperatively. op.: operation, MMA: middle meatal antrostomy. 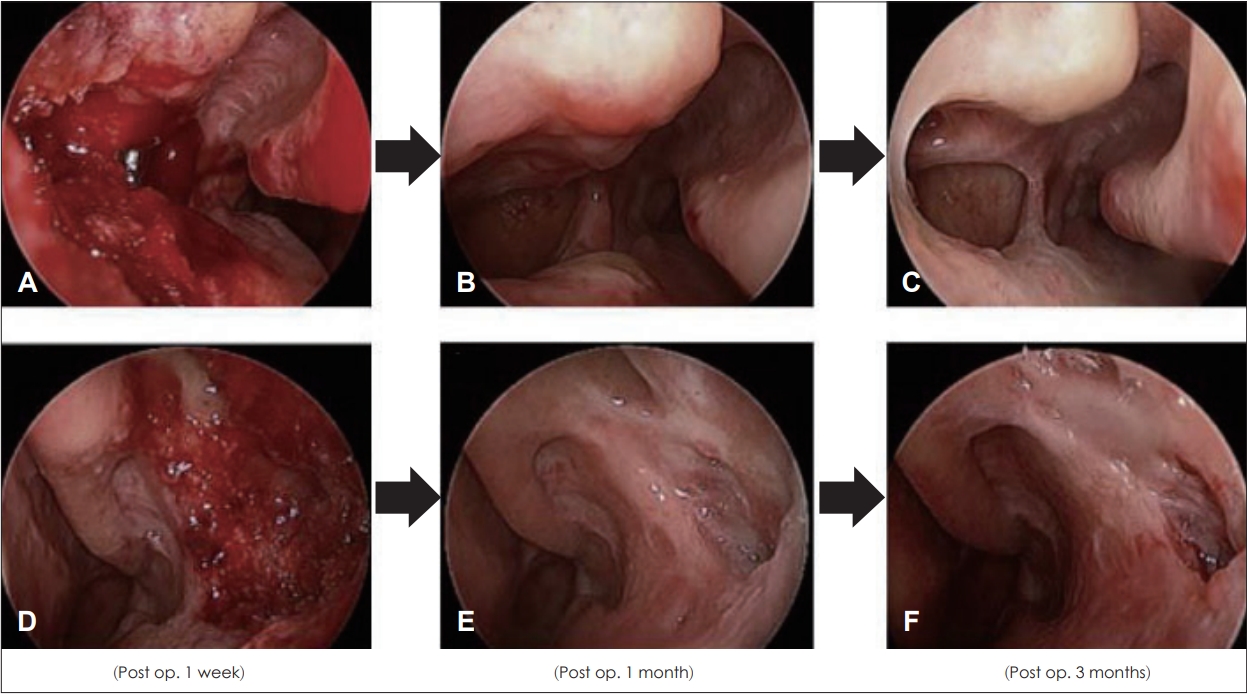
Fig. 2.
Classification of Grade I to IV according to endoscopic and CT findings. Grade I shows nothing significant on the endoscope and only haziness at the maxillary sinus floor on CT (A). Grade II shows mucopus on endoscope and haziness extending to the middle portion of the maxillary sinus on CT (B). Grade III has haziness extended to the natural ostium of the maxillary sinus (C), and Grade IV has extra sinus extension to the ostiomeatal unit area on CT (D). 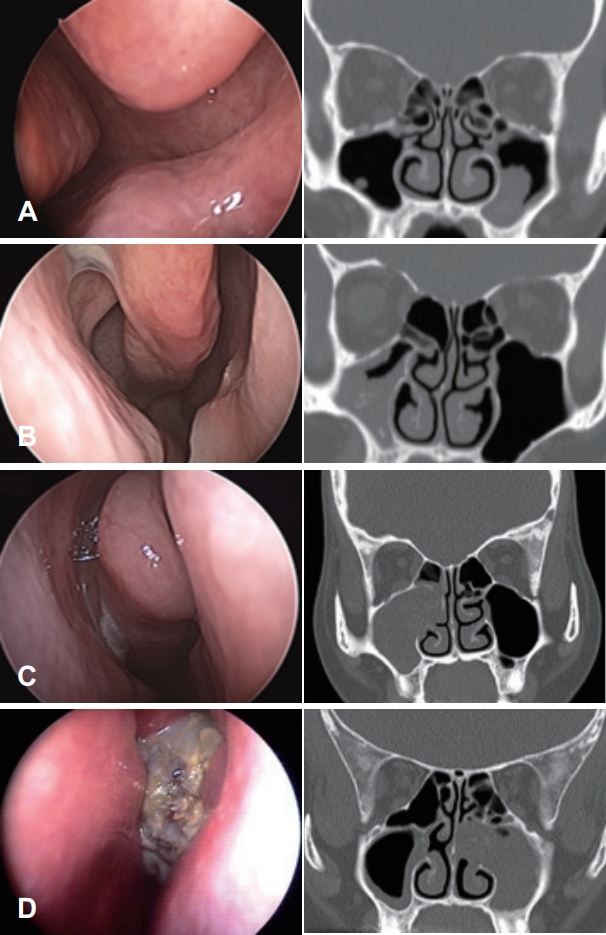
Fig. 3.
Overall recovery periods of fungus ball. When classified according to grade, Grade 1 showed the shortest recovery time i.e., 10.5±2.8 weeks, and Gade IV showed the longest time, i.e., 16.3± 6.8 weeks. In other words, the higher the grade, the fungus balls were more closely located to the natural ostium of the maxillary sinus and the recovery time tended to become longer with statistical significance (p=0.001). 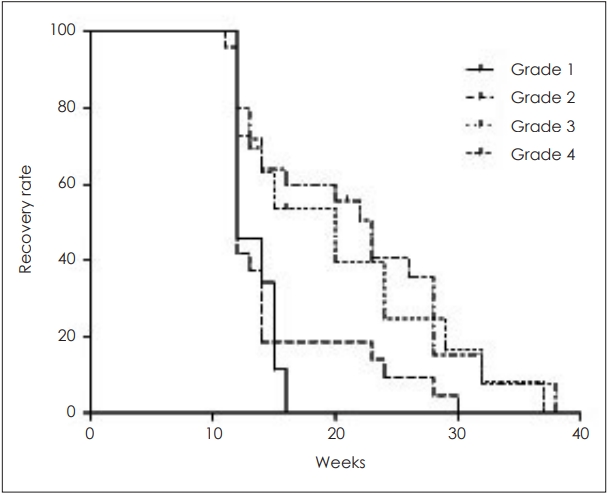
Table 1.
Demographic data and comorbidities of patients with fungus ball
|
Variables |
No. of patients (%) |
|
Age (years) |
60.9±11.8 (28-85) |
|
Male:female |
55:110 (33:67) |
|
Unilateral:bilateral |
158:7 (95.8:4.2) |
|
Allergic rhinitis (Y:N) |
26:139 (15.8:84.2) |
|
Diabetes mellitus (Y:N) |
29:136 (17.6:82.4) |
|
Asthma (Y:N) |
3:162 (1.8:98.2) |
|
Alcohol (Y:N) |
38:127 (23:77) |
|
Smoking (Y:N) |
12:153 (7.3:92.7) |
Table 2.
Relation between fungus ball extension Grade and demographic data and comorbidities
|
Grade I (n=23, %) |
Grade II (n=38, %) |
Grade III (n=67, %) |
Grade IV (n=37, %) |
p value |
|
Age |
63.5±10.0 |
59.3±11.6 |
60.97±12.3 |
60.85±11.8 |
0.619 |
|
Sex (M:F) |
7:16 |
9:29 |
22:45 |
17:20 |
0.227 |
|
Follow up (weeks) |
10.8±6.9 |
13.5±8.0 |
12.54±7.0 |
15.43±8.5 |
0.140 |
|
Allergic rhinitis |
1 (4.3) |
8 (21) |
10 (14.9) |
7 (18.9) |
0.337 |
|
Bone thickness |
15 (65.2) |
26 (68.4) |
48 (71.6) |
28 (75.7) |
0.825 |
|
Dental problem |
11 (47.8) |
23 (60.5) |
42 (64.2) |
23 (63.2) |
0.579 |
|
Operation time (minute) |
32.3±14.7 |
30±12.7 |
30.5±17.8 |
35.1±13.7 |
0.484 |
|
Estimated blood loss (mL) |
20.2±18.3 |
37.5±21.1 |
24.3±20.8 |
30.2±28.8 |
0.821 |
|
Diabetes mellitus |
4 (17.4) |
5 (13.2) |
10 (14.9) |
10 (27.0) |
0.374 |
|
Asthma |
0 |
1 (2.6) |
1 (1.5) |
1 (2.7) |
0.857 |
|
Alcohol |
1 (4.3) |
7 (18.4) |
18 (26.9) |
12 (32.4) |
0.061 |
|
Smoking |
0 |
0 |
5 (7.5) |
7 (18.9) |
0.007 |
Table 3.
Distribution of chief complaints in patients with fungus ball according to fungus ball extension Grade
|
Grade I (n=23, %) |
Grade II (n=38, %) |
Grade III (n=67, %) |
Grade IV (n=37, %) |
|
No symptoms |
8 (34.8) |
12 (31.6) |
6 (9) |
4 (10.8) |
|
Postnasal drip |
7 (30.4) |
7 (18.4) |
10 (14.9) |
2 (5.4) |
|
Headache |
3 (13.0) |
4 (10.5) |
12 (17.9) |
7 (19) |
|
Foul odor |
2 (8.7) |
1 (2.6) |
5 (7.5) |
3 (8.1) |
|
Facial pain/fullness |
1 (4.3) |
2 (5.3) |
9 (13.4) |
3 (8.1) |
|
Nasal obstruction |
1 (4.3) |
7 (18.4) |
9 (13.4) |
10 (27.0) |
|
Purulent rhinorrhea |
1 (4.3) |
5 (13.2) |
13 (19.4) |
5 (13.5) |
|
Etc. |
0 (0) |
0 (0) |
3 (4.5) |
3 (8.1) |
Table 4.
Relation between fungus ball extension Grade and dental health conditions
|
Grade I (n=23, %) |
Grade II (n=38, %) |
Grade III (n=67, %) |
Grade IV (n=37, %) |
p value |
|
Normal |
12 (52.2) |
15 (39.5) |
24 (35.8) |
14 (37.8) |
0.579 |
|
Dental prosthesis |
10 (43.5) |
21 (55.3) |
34 (50.7) |
16 (43.2) |
0.694 |
|
Implant |
0 (0) |
1 (2.6) |
7 (10.4) |
2 (5.4) |
0.207 |
|
Periapical abscess |
1 (4.3) |
1 (2.6) |
2 (3.0) |
5 (13.5) |
0.107 |
Table 5.
Relation between fungus ball extension Grade and prognosis, wound healing and touch up
|
Grade I (n=23) |
Grade II (n=38) |
Grade III (n=67) |
Grade IV (n=37) |
p value |
|
Good |
22 |
36 |
55 |
23 |
|
|
Poor |
1 |
2 |
12 |
14 |
|
|
Wound healing (%) |
95.7 |
94.7 |
82 |
62.1 |
0.005 |
|
Touch up |
1 |
1 |
4 |
4 |
|
|
Clinical outcome (%) |
95.65 |
97.36 |
94.02 |
89.18 |
0.251 |
Table 6.
Outpatient clinic follow up period according to fungus ball extension Grade
|
Grade I (n=23) |
Grade II (n=38) |
Grade III (n=67) |
Grade IV (n=37) |
p value |
|
Weeks |
10.5±2.8 |
10.9±3.6 |
15.1±6.7 |
16.3±6.8 |
0.001 |
REFERENCES
1. Stammberger H. Endoscopic surgery for mycotic and chronic recurring sinusitis. Ann Otol Rhinol Laryngol Suppl 1985;119:1-11.   2. Nicolai P, Lombardi D, Tomenzoli D, Villaret AB, Piccioni M, Mensi M, et al. Fungus ball of the paranasal sinuses: Experience in 160 patients treated with endoscopic surgery. Laryngoscope 2009;119(11):2275-9. 4. Kennedy DW. Prognostic factors, outcomes and staging in ethmoid sinus surgery. Laryngoscope 1992;102(12 Pt 2 Suppl 57):1-18.
5. Klossek JM, Serrano E, Péloquin L, Percodani J, Fontanel JP, Pessey JJ. Functional endoscopic sinus surgery and 109 mycetomas of paranasal sinuses. Laryngoscope 1997;107(1):112-7. 6. Lop-Gros J, Gras-Cabrerizo JR, Bothe-González C, MontserratGili JR, Sumarroca-Trouboul A, Massegur-Solench H. Fungus ball of the paranasal sinuses: Analysis of our serie of patients. Acta Otorrinolaringol Esp 2016;67(4):220-5. 9. Pagella F, Matti E, De Bernardi F, Semino L, Cavanna C, Marone P, et al. Paranasal sinus fungus ball: Diagnosis and management. Mycoses 2007;50(6):451-6. 10. Ferguson BJ. Fungus balls of the paranasal sinuses. Otolaryngol Clin North Am 2000;33(2):389-98. 11. deShazo RD, O’Brien M, Chapin K, Soto-Aguilar M, Swain R, Lyons M, et al. Criteria for the diagnosis of sinus mycetoma. J Allergy Clin Immunol 1997;99(4):475-85. 15. Johnson K, Parham K. Nasal and paranasal sinus infections. In: James R. Hupp, Elie M. Ferneini, eds. Head, Neck and Orofacial Infections: An Interdisciplinary Approach E-Book. Amsterdam: Elsevier Health Sciences; 2015. p. 248.
|
|














