서 론
내시경이 소개된 이후로 내시경 부비동 수술이 상악동을 포함하는 비부비동 질환을 치료하는 데 근간이 되어왔다. 그러나 상악동은 피라미드 모양의 방추형 공간으로, 내시경 발달과 다양한 기구 개발에도 해부학적 이유로 상악동의 내벽, 전벽의 접근이 어려워 이곳에 병변이 있을 때 제거하기가 용이하지 않다[1,2].
반전성 유두종은 가장 흔한 비부비동 양성종양으로 상악동에서 잘 발생하며, 종양 부착 부위를 잘 제거하는 것이 재발 방지를 위해 매우 중요하다. 그래서 반전성 유두종의 흔한 재발은 불완전한 외과적 절제와 관련이 있다[3]. 상악동 반전성 유두종 수술에는 중비도 개창술, Caldwell-Luc 수술, 견치와 천자(canine fossa puncture), 내시경하 상악골 내측절제술이 시행되어 왔다[4-8]. 최근까지 상악동 반전성 유두종에서 내시경하 상악골 내측절제술이 가장 일반적으로 사용되는 내시경적 접근방법이었다. 그러나 상악동 내벽을 절제하는 내시경하 상악골 내측절제술으로도 상악동내의 전누골와(prelacrimal recess)과 치조함요(alveolar recess)의 병변 제거가 어렵고, 하비갑개와 비루관(nasolacrimal duct)을 절제가 포함된다[1,9].
Zhou 등[10]은 전누골와 접근법을 처음 소개하였으며, 이 방법에는 두 가지 장점이 있다. 첫째, 전누골와와 상악동 전벽을 포함하여 상악동 내의 전체적인 시야가 확보되어 병변제거가 용이하다는 장점과, 둘째로는 하비갑개와 비루관의 절제를 포함하는 고식적인 내시경하 내측 상악골 절제술과는 달리 하비갑개와 비루관의 보존이 가능한 술식이라는 점이다.
비루관은 누낭(lacrimal sac)으로부터 하비도로 이어지는데 골내(interosseous) 부분과 비도내(intrameatal) 부분으로 구성되어 있다. 비루관은 제2 소구치 뒤 가장자리 혹은 제1 대구치를 향해 아래, 뒤, 그리고 외측으로 향하며, 이러한 경로는 비강 외측벽과 관련되기 때문에 비강 외측벽을 제거하는 술식에서 비루관의 해부학적 구조에 대한 이해가 필요하다[11].
본 연구의 목적은 비루관 하부와 주변 구조물과의 관계를 부비동 전산화단층횔영(CT)을 이용한 계측을 통해 전누골와 접근법과 같은 비루관의 보존이 필요한 수술에서의 참고 자료로 활용하고자 하였다.
대상 및 방법
대 상
2018년 3월부터 2021년 5월까지 본 병원에 비과적 증상으로 내원하여 부비동 CT를 촬영했던 총 1907명 중에서 1) 상악동 병변(종양, 진균성 부비동염, 팽창성 종물, 폴립 등)이 있는 경우, 2) 코 수술 기왕력(부비동 내시경 수술 또는 Caldwell-Luc 수술)이 있는 경우, 3) 과거 안면 골절로 변형이 있는 경우, 4) 병력상 비루관 질환이 있거나 비루관 수술 기왕력이 있는 경우, 5) 18세 미만의 경우는 제외하였다. 연구대상군은 총 276명(남자 151명, 여자 125명)으로 각각 양측 552측에 대해 연구를 수행하였다. 전체 평균나이는 남자는 45.3±14.9세였고, 여자는 43.1±15.8세였다. 본 연구는 원광대학교병원 기관심의위원회의 승인(2021-11-009)을 받고 수행되었다.
부비동 단층촬영 분석
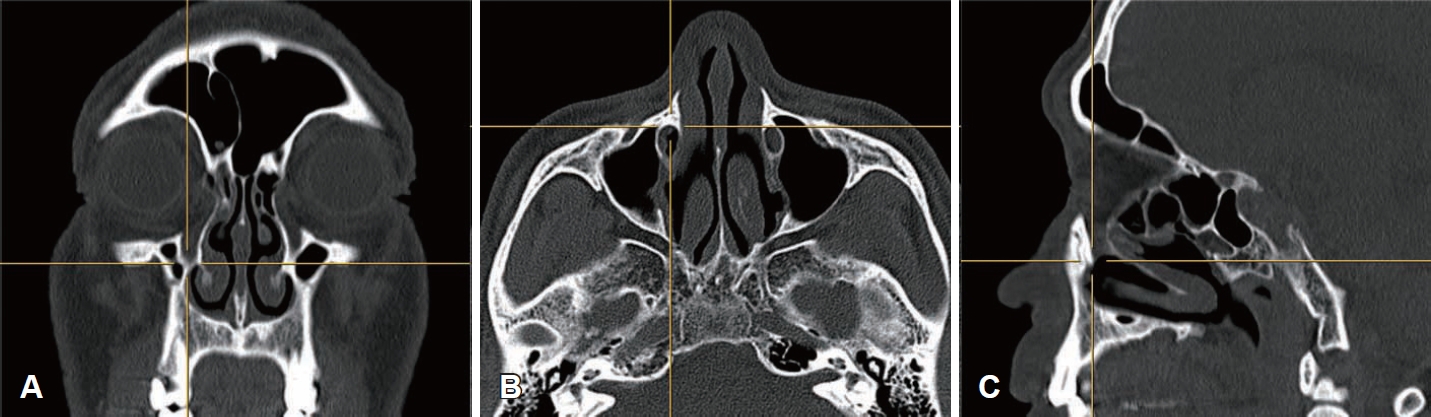
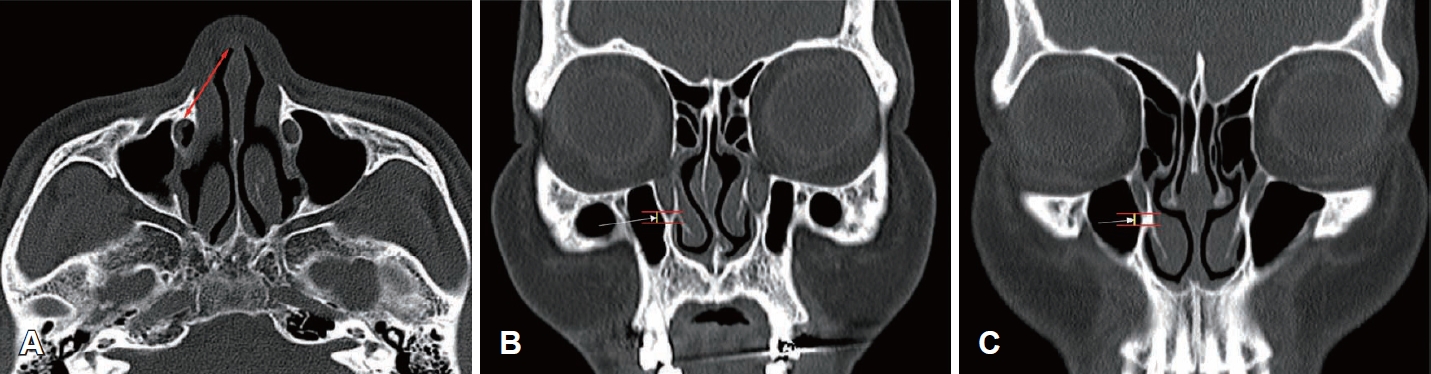
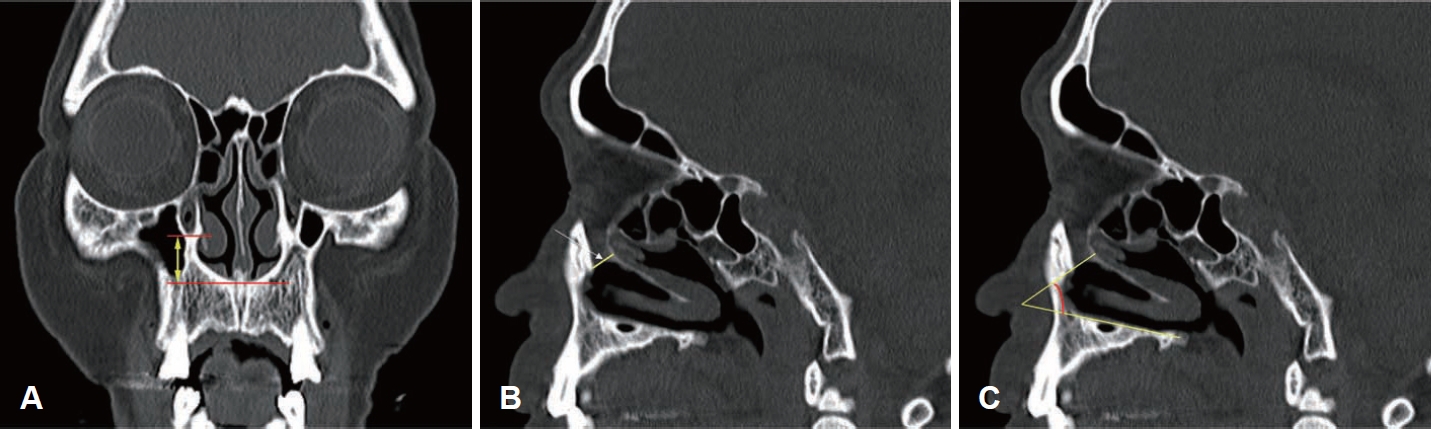
부비동 CT의 시상면(sagittal), 관상면(coronal), 축면(axial) 영상을 이용하였는데, 관상면 영상에서 비루관의 골성 부위 영상을 기준으로 비루관의 하단에 3차원 커서를 적용한 후, 그 지점에 해당되는 시상면, 축면 영상을 나타내어 다음과 같은 5가지 거리를 측정하였다(Fig. 1). 1) 축면 영상에서 비공(nostril)와 비루관 하단의 가장 앞 부위와의 거리(Fig. 2A), 2) 관상면 영상에서 하비갑개의 비강 외측 벽 부착부위를 기준으로 비루관의 하단이 하비갑개의 외측 벽 부착부위의 하방에 있을 경우 양값(+), 상방에 있을 경우 음값(-)으로 표시한 거리(Fig. 2B and C), 3) 관상면 영상에서 비루관의 하단과 비강저(nasal cavity floor)까지의 거리(Fig. 3A), 4) 시상면 영상에서 비루관 하단의 전후 직경(하단에서 전면부터 후면까지의 가장 짧은 거리) (Fig. 3B), 5) 시상면 영상에서 비루관 하단의 전후 직경 연장선과 비강저와의 각도(Fig. 3C)를 측정하였고, 각각 좌우에서 시행하였다.
결 과
비공과 비루관 하단의 가장 앞 부위와의 거리
연구대상군 276명 중 151명의 남자 우측 평균은 28.32±3.44 mm, 125명의 여자 평균은 24.19±2.55 mm였고, 남자 좌측 평균은 27.45±3.88 mm, 여자 평균은 24.14±2.69 mm였다. 연구대상군 276명의 우측 평균은 26.45±3.69 mm, 좌측은 25.95±3.77 mm로 양측 간의 유의한 차이를 보였다(p=0.012) (Table 1).
하비갑개의 외측 벽 부착부위를 기준으로 비루관의 하단 부위까지 거리
연구대상군 276명 중 151명의 남자 우측 평균은 1.58±2.22 mm, 125명의 여자 평균은 1.10±1.83 mm였고, 최저값과 최대값은 각각 -5.43 mm, 7.75 mm였다. 남자 좌측 평균은 1.14±1.85 mm, 여자 평균은 0.79±1.87 mm였고, 최저값과 최대값은 각각 -5.30 mm, 5.51 mm였다. 연구대상군 276명의 우측 평균은 1.36±2.07 mm, 좌측은 0.98±1.86 mm로 양측 간의 유의한 차이를 보였다(p=0.003) (Table 1).
비루관의 하단과 비강저와의 거리
연구대상군 276명 중 151명의 남자 우측 평균은 18.21±3.72 mm, 125명의 여자 평균은 16.41±2.85 mm였고, 남자 좌측 평균은 18.16±3.03 mm, 여자 평균은 16.74±3.13 mm였다. 연구대상군 276명의 우측 평균은 17.39±3.46 mm, 좌측은 17.52±3.15 mm로 양측 간의 유의한 차이를 보이지 않았다(p=0.462) (Table 1).
비루관 하단의 전후 직경
연구대상군 276명 중 151명의 남자 우측 평균은 7.77±1.72 mm, 125명의 여자 평균은 8.03±1.57 mm였고, 남자 좌측 평균은 7.88±1.47 mm, 여자 평균은 8.06±1.73 mm였다. 연구대상군 276명의 우측 평균은 7.89±1.66 mm, 좌측은 7.96±1.60 mm로 양측간의 유의한 차이를 보이지 않았다(p=0.395) (Table 1).
비루관 하단의 직경 연장선과 비강저와의 각도
연구대상군 276명 중 151명의 남자 우측 평균 각도는 46.08°±11.18°, 125명의 여자 평균은 47.43°±8.24°였고, 남자 좌측 평균 각도는 44.32°±10.77°, 여자 평균은 45.90°±9.56°였다. 연구대상군 276명의 우측 평균은 46.69°±9.97°, 좌측은 45.04°±10.25°로 양측 간의 유의한 차이를 보였다(p=0.006) (Table 1).
연령과 각 측정값과의 상관성(Table 2)
1) 연령과 측정값 1 (비공과 비루관 하단의 가장 앞 부위와의 거리)과는 음적인 상관관계를 보였다(r=-0.191, p<0.001).
2) 연령과 측정값 2 (하비갑개의 비강 외측 벽 부착부위를 기준으로 비루관의 하단까지 거리)와는 양적인 상관관계를 보였다(r=0.094, p=0.028).
3) 연령과 측정값 3 (비루관의 하단과 비강저와의 거리)과는 음적인 상관관계를 보였다(r=-0.194, p<0.001).
4) 연령과 측정값 4 (비루관 하단의 전후 직경)와는 양적인 상관관계를 보였다(r=0.136, p=0.001).
5) 연령과 측정값 5 (비루관 하부의 직경 연장선과 비강저와의 각도)와는 상관관계를 보이지 않았다(p=0.150).
고 찰
비루관 손상은 내시경 부비동 수술에서 발생 가능한 합병증으로서, 1.7%에서 15%까지 다양하며, 이는 수술 의사의 비루관에 대한 해부학적 지식 부족과 관련이 있을 수 있다[12].
상악동에 대한 하비도 접근법은 내시경 조직 검사를 수행하거나 상악동의 내하측에 위치한 상악동 병변 혹은 이물제거에 유용하다[13]. 45도 또는 70도 내시경을 사용하면 하비도 내의 비루관 개구부를 확인 가능하기 때문에 안전하게 하비도 개창술을 시행할 수 있다.
Zhou 등[10]이 처음 소개한 전누골와 접근법은 전누골와와 상악동 전벽의 시야를 위해 비루관을 하비갑개와 같이 내측으로 이동함으로써 하비도 개창술과 달리 비루관과 주변 구조물과의 해부학적 지식이 중요하다.
비루관의 개구부는 하비도에서 다양한 높이에 위치하고 작은 개구부로부터 큰 개구부에 이르기까지 크기가 매우 다양하고, 모양도 둥근 모양부터 슬릿(slit) 모양까지 다양하다. 개구부가 하비도에서 높은 위치에 있을 때는 개구부의 폭이 넓은 경향이 있으며, 아래쪽에 위치할 때는 슬립 모양인 경우가 많다[14].
Lang [15]은 성인의 비루관 개구부가 비강 입구로부터 22 mm와 25 mm 사이에 있다고 보고했다. 본 연구에서 남자에서 여자보다 길게 측정되었으며, 우측 평균은 26.45±3.69 mm, 좌측은 25.95±3.77 mm로 Lang의 연구와는 큰 차이는 보이지 않았다. Yanagisawa와 Yanagisawa [16] 연구에서 비루관 개구부가 비강저보다 약 1.5 cm 상방에 위치하였는데, 본 연구에서는 비루관 하단이 남자에서 여자보다 높게 측정되었으며, 우측 평균은 17.39±3.46 mm, 좌측은 17.52±3.15 mm였다.
Lang [15]과 Orhan 등[14]의 연구에서는 사체연구에서 성인의 비루관 개구부가 하비도의 상부로부터 각각 5.75 mm, 5.0 mm 떨어진 곳에 위치한다고 보고했다. 본 연구에서는 전누골와 접근법에서 중요한 지표인 하비갑개의 비강 외측 벽 부착부위를 기준으로 비루관의 하단이 하비갑개의 외측 벽 부착부위의 하방에 있을 경우 양값(+), 상방에 있을 경우 음값(-)으로 표시하여 거리를 측정하여 평균을 구한 결과, 우측 평균은 1.36±2.07 mm, 좌측은 0.98±1.86 mm였다.
Lang [15]의 연구에서는 비루관 개구부의 전후 직경을 측정했는데 평균 6.4 mm였다. 본 연구는 시상 영상에서 비루관 하단의 전후 직경을 측정하였는데 우측 평균은 7.89±1.66 mm, 좌측은 7.96±1.60 mm로 양측 간의 유의한 차이를 보이지 않았다. 이러한 결과는 사체 해부 연구와 부비동 CT를 이용한 연구 방법에 따른 차이와 인종 간의 차이일 수 있다.
Unlu¨ [17]와 Orhan 등[14]의 연구에서 비강관 개구부와 전비극(anterior nasal spine)의 평균 각도는 각각 35.8°, 33.2°였다. 본 연구는 비루관 하단의 전후 직경 연장선과 비강저와의 각도로 우측 평균은 46.69°±9.97°, 좌측은 45.04°±10.25°였다. 비강 측벽에 부착된 하비갑개의 전면부는 비강저와 30°-45°를 형성한다. 연구들 간에 방법론에서 차이가 있을 수 있으나 45° 내시경을 사용하면 하비도 내에서의 비루관 개구부의 관찰이 가능하다.
비공과 비루관 하단의 가장 앞 부위와의 거리, 하비갑개의 비강 외측 벽 부착부위에서 비루관의 하단 부위까지의 거리, 비루관 하단의 직경 연장선과 비강저와의 각도에서 양측이 유의하게 차이를 보였으며, 그에 대한 정확한 이유는 알 수 없었으나, 두개안면 해부학 연구에서 두개골의 비대칭은 성인에서 흔히 관찰되는 소견이다[18,19].
연령과 5가지의 측정값과의 상관관계 분석에서 연령과 측정값 1, 3번은 음적인 상관 관계를 보였는데, 이는 노화에 따른 안면골의 리모델링과 연관성이 있어 측정거리가 감소되었을 것으로 보인다[20].
본 연구의 강점으로는 처음으로 부비동 CT를 이용하여 276명(552측)의 한국인을 대상으로 한 비루관 하단과 주변 구조물과의 계측을 한 연구로서 임상적 적용을 위한 기초 자료로 활용될 수 있다. 특히 전누골와 접근법에서 중요한 지표인 하비갑개의 비강 외측 벽 부착부위를 기준으로 비루관의 하단이 하비갑개의 외측 벽 부착부위에 평균적으로 1 mm 내외로 측정되었으나, 측정값의 범위는 -5.51 mm에서 +7.75 mm로 개인 간의 차이를 보일 수 있어 수술 시에 면밀한 CT 검토가 필요하다. 본 연구의 제한점으로는 사체 연구가 아닌 CT 계측치로 수술 시 본 연구의 결과를 그대로 적용하기에는 한계가 있을 수 있어 참고 자료로 활용되기를 기대한다.
본 연구의 결과를 요약하면, 한국인에서 부비동 CT의 영상학적 계측을 통해 평균적으로 비공으로부터 비루관 하단이 25 mm, 45도 각도로 존재하며, 비강저로부터는 17 mm 상방에 존재하며, 비루관 하단의 전후 직경은 약 8 mm였다. 하비갑개의 비강 외측 벽 부착부위를 기준으로 비루관의 하단이 부착부위에 인접해 있으나 개인차가 있을 수 있다.