성대 백반증의 혈관용해 레이저 수술 후 2D 스캐닝 디지털 카이모그래피를 이용한 성대 진동 변화의 양적 평가
Abstract
Background and Objectives
Vocal fold leukoplakia is characterized as white plaque on the epithelium of the vocal folds and can be treated by angiolytic laser stripping surgery. However, postoperative changes in the vibratory patterns of vocal folds have not been investigated quantitatively. The purpose of this study was to investigate the changes in vocal fold vibration after angiolytic laser surgery in patients with unilateral vocal fold leukoplakia using the twodimensional scanning digital kymography (2D DKG).
Subjects and Method
Medical records of seven males (age=62.14±12.40 yrs) with unilateral vocal fold leukoplakia who underwent angiolytic laser stripping were reviewed. Before and after the surgery (post-operative day=82.57±28.55 days), a multi-dimensional voice assessment was performed along with a 2D DKG study. For 2D DKG images, the amplitude symmetry index (ASI), phase symmetry index (PSI), and open quotient (OQ) were calculated using the ImageJ program. In addition, pre- versus postoperative data were compared, and the correlation between the changes in 2D DKG parameters and voice outcomes was explored.
Results
Results indicated that the absolute ASI (p=0.028) and OQ (p=0.028) of the 2D DKG study, grade (p=0.038) and breathy (p=0.034) of the GRBAS scale, σPitch measured by the electroglottography (p=0.043), the physical score of the VHI (p=0.042), and the total score (p=0.043) and the tiredness score (p=0.043) of the VFI decreased after surgery. Decrease in the absolute ASI was correlated with changes in the grade (rho=0.850) and breathy (rho=0.777) scale measures, while decreased OQ were correlated with the changes in the physical score of the VHI (rho=0.901) and tiredness score of the VFI (rho=0.847).
Conclusion
The improved vocal fold vibratory patterns after angiolytic laser surgery for vocal fold leukoplakia can be evaluated objectively using the 2D DKG study. Angiolytic laser stripping enables the preservation of vocal fold vibration after the surgery and is considered a valuable surgical option for treating vocal fold leukoplakia.
Key words: Kymography ㆍ Lasers ㆍ Leukoplakia ㆍ Vibration ㆍ Vocal cords
서 론
성대 백반증(vocal fold leukoplakia)은 마찰로 쉽게 제거되지 않는 성대 표피의 전암성 백색 피부 병변으로 과각화증(hyperkeratosis), 이형성증(dysplasia), 편평상피세포암 등의 다양한 병리 소견을 보인다. 1960년도부터 2005년까지 후두 백반증을 보인 환자 2188명을 대상으로 한 연구에서 50%는 과각화증과 같은 양성 병변으로 밝혀졌으며 나머지 50%는 이형성증을 보이는 전암성, 혹은 악성 병변으로 밝혀졌다[ 1]. 전암성 병변의 8.2%는 악성으로의 진행을 보이며 이형성증의 정도와 악성으로의 변화율이 유의미한 관계를 보인다. 비록 성대 백반증이 악성으로의 변화 가능성을 내재하였더라도 상대적으로 높은 양성의 가능성과 낮은 악성 변화율을 보일 뿐만 아니라, 과도한 절제는 성대점막의 상처로 인한 영구적인 음성장애를 유발할 수 있기 때문에 수술적 절제범위는 신중하게 결정하여야 한다. 수술적 치료로는 고식적 절제술 혹은 CO 2 레이저, 혈관용해 레이저(angiolytic laser) 등 다양한 레이저를 사용한 방법이 있으며, 수술 범위에 따라 소작술(vaporization), 거상술(stripping), 절제술(resection) 등의 수술적 방법이 사용되고 있다. 이 중 혈관용해 레이저는 혈색소에 선택적으로 흡수되는 레이저 광선을 이용하여 혈액이 풍부한 조직에 혈관용해를 일으킴으로써 정상 조직에 대한 보존과 함께 세밀함을 요하는 후두미세수술에 적합한 레이저로 대두되고 있다. 저자들은 최근 최소침습적 절제면을 확보할 수 있는 레이저 절제술 또는 거상술을 이용하여 음성 보존에서 좋은 결과를 보고하였다[ 2]. 성대 백반증으로 CO 2 레이저를 이용한 후두미세수술과 혈관용해 레이저를 이용한 수술을 시행받은 환자군 간의 치료 결과를 비교하였을 때, 두 치료군 간에 재발 혹은 악성 변환에 대한 차이는 보이지 않았으며, 음성의 보존에 있어서는 혈관용해 레이저를 이용한 환자군이 더 우세함을 보였다[ 2]. 그러나 레이저 수술 후 성대 진동 양상에 대한 정량적 평가는 아직까지 연구된 바 없다. 성대 진동 특성에 평가와 점막파동에 대한 정량적 계산 방법으로 후두 스트로보스코피(laryngeal stroboscopy), 고속 후두내시경 검사(high-speed videolaryngoscopy), 카이모그래피(kymography) 등을 사용할 수 있다[ 3]. 이 중 2D 디지털 카이모그래피(two-dimensional scanning digital kymography, 2D DKG)는 불안정한 발성 상태에서도 측정이 가능하며 측정된 성대 점막의 움직임을 시각화하여 표현할 수 있다는 점에서 성대 진동 평가에 장점을 가지며, 최근 자동화된 분석을 통한 정량적 측정도 가능해지고 있다[ 4, 5]. 또한 고속촬영법을 이용하여 성대의 모든 움직임을 관측할 수 있는 유일한 방법으로 성대 반흔(vocal fold scarring) 혹은 성대 위축(vocal fold atrophy) 등에서 유용성이 보고된 바 있다[ 6, 7]. 성대 백반증과 같이 불규칙한 성대점막 진동패턴을 보이는 질환에서의 성대진동 패턴 분석에 강점을 가질 수 있다. 본 연구에서는 혈관용해 레이저 거상술을 시행받은 성대 백반증의 환자들에게 2D DKG를 사용하여 진폭대칭지수(amplitude symmetry index, ASI), 위상대칭지수(phase symmetry index, PSI), 개방지수(open quotient, OQ)의 정량적 변화를 측정, 비교분석하여 혈관용해 레이저를 사용한 성대 백반증 거상술의 수술 후 성대진동 양상의 호전 정도를 비교하였다. 또한 2D DKG에서의 소견과 음성 호전 양상의 비교를 통해 성대 진동에 대한 정량적 측정 도구로서의 가치를 평가해 보았다.
대상 및 방법
대 상
음성장애를 주소로 본원에 내원하여 이비인후과 전문의에 의해 성대 백반증으로 진단된 환자 중 전신마취하에 혈관용해 레이저 거상술을 시행받았던 7명의 성인 남성(62.14±12.40세)을 대상으로 진행하였다. 다른 후두 질환을 동반하거나 이전에 후두 미세수술이나 방사선 치료를 받은 병력이 있는 환자는 제외하였다. 본 연구는 후향적 연구의 형태로 진행되었으며 기관연구윤리심의위원회(Institutional Review Board No. 3-2020-0280)의 승인을 받았다( Table 1).
수술 방법
수술은 전신마취하에 진행되었다. Dedo 후두경을 이용하여 진성대를 노출시켰으며 수술 현미경을 통해 시야확보 후 532 nm 혈관용해 레이저(QUANTA D562-6, Quanta System SpA, Samarate, Italy)의 광섬유(laser fiber)를 악구겸자(alligator forceps)를 이용하여 병변을 향하도록 하였다. 광섬유의 끝부분이 병변의 3 mm 이내의 범위 안에서 이동하며 일반적인 경우 병변 전체에 레이저를 비접촉성 모드(noncontacting mode)로 4 watt, 20 Hz 사용했으며 필요 시 5 watt의 세기로 전달하였다. 혈관용해 레이저는 상피 밑의 미세혈관을 용해하여 고유층의 표면(superficial lamina propria)과 상피(epithelium)를 분리하였으며 이후 나타난 병변의 기저막(basal membrane)과 상피(epithelium) 사이의 단면을 악구겸자와 솜뭉치(cotton ball)를 이용하여 거상시켜 미세피판의 일괄절제술(en-bloc resection)을 시행하였다. 이후 검체는 병리과로 운반되어 병리학적 진단 과정을 거쳤다( Fig. 1).
2D 디지털 카이모그래피 분석
수술 후 추적 관찰은 82.57±28.55일간 진행되었으며, 5인의 대상자(증례 1, 2, 4, 5, 6)는 술후 3개월경, 2인(증례 3, 7)은 술후 1개월경에 시행하였다. 다기능후두검사시스템(multidimensional examination system; USC-700MF; U-Medical, Busan, Korea)과 70°경성 내시경(8700 CKA; Karl Storz, Tuttlingen, Germany)을 사용하여 성대를 촬영하였다. 촬영한 영상은 정량적 분석을 위해 2픽셀 라인 스캐닝을 사용하여 2D 디지털 카이모그래피를 구현하였다[ 5]. 2D 디지털 카이모그래피 분석 시 이미지가 변형되는 것을 방지하기 위해 Adobe Illustrator (Adobe Systems Inc., San Jose, CA, USA) 프로그램에서 벡터화(vectorize)를 실시한 후, ImageJ program (U. S. National Institutes of Health, Bethesda, MD, USA) 1.52a에서 8 bit gray scale로 변환하여 수술 전후 ASI, PSI, OQ를 측정하였다( Fig. 2). 추가적인 음성 분석을 위해 수술 전후 모음연장발성에서 음향학적 평가방법인 Analysis of Dysphonia Speech and Voice (ADSV) (Model 5109; KayPENTAX, Lincoln Park, NJ, USA)를 이용하여 켑스트럼 피크 현저성(cepstral peak prominence, CPP), L/H 스펙트럼 비율(L/H spectral ratio, SR), σCPP, σSR을, Multi-Dimensional Voice Program (MDVP) (Model 5105, KayPENTAX)을 이용하여 주파수변동율(jitter percent), 진폭변동율(shimmer percent), 소음 대 배음 비율(noise-to-harmonic ratio)을 측정하였다. 전기성문파형검사(electroglottography, EGG)로는 realtime EGG analysis (Model 5138; KayPENTAX)를 이용하여 수술 전후 문단읽기에서의 발화 기본주파수(speaking fundamental frequency, SFF), 성문접촉률(contact quotient, CQ), σSFF, σCQ를 측정하였다.
또한 7점 척도의 GRBAS를 이용하여 수술 전후 모음연장 발성 및 문단읽기에서의 청지각적 평가를 실시하였으며[ 8], 한국판 음성장애지수(Korean version of Voice Handicap Index, KVHI)와 한국판 음성피로지수(Korean version of Vocal Fatigue Index, K-VFI) 설문지를 통해 주관적 음성평가도 실시하였다[ 9, 10].
통계 분석
수술 전후의 음성 비교는 윌콕슨 부호순위 검정(Wilcoxon signed rank test)을 사용하였다. 수술 전후 2D DKG 측정변수의 변화량과 음성변수의 변화량 간의 상관관계는 스피어만 상관분석(Spearman correlation)을 사용하여 알아보았다. 유의 수준은 0.05로 설정하였다.
결 과
7명 환자의 조직학적 검사 결과 6명의 환자가 과각화증 소견을 보였으며 1명의 환자가 이형성증 소견을 보였다. 1명의 환자가 양측성의 백반증을, 6명의 환자가 일측성 백반증을 보였으며 각각 3명씩 우측과 좌측에서의 백반증을 보였다. 술후 추적 관찰 중 1명의 환자가 백반증의 재발 소견을 보여 혈관용해 레이저를 이용한 거상술을 재시행하였다.
환자들의 수술 전과 후의 검사들에 대하여 분석한 결과 2D DKG에서의 ASI ( p=0.028), OQ ( p=0.028)에서의 통계적으로 유의한 향상 소견을 보였으며( Fig. 3) GRBAS 중 grade ( p=0.038), breathy ( p=0.034)에서 유의미한 감소를 보였다. ADSV와 MVDP의 분석 변수들 가운데에는 유의한 차이를 보인 변수가 없었던 반면, EGG상에서는 σSFF ( p=0.043)에서의 감소를 보였고, KVHI에서는 신체 점수(physical, p=0.042)가, K-VFI에서는 총점( p=0.043)과 피로감 점수(tiredness, p=0.043)가 유의미한 감소를 보였다. 2D DKG의 측정 변수와 음성 측정 변수의 변화량 간 상관관계를 살펴본 결과, 감소된 ASI의 변화량(ΔASI)은 GRBAS의 Δgrade (rho=0.850)와 Δbreathy (rho=0.777)와 양의 상관관계를 보였으며 감소된 ΔOQ는 KVHI의 Δphysical (rho=0.901)과 K-VFI의 Δtiredness (rho=0.847)와 양의 상관관계를 보였다( Fig. 4 and Table 2).
고 찰
성대 백반증은 병리학적 진단명이 아닌 임상소견에 대한 명칭으로, 전암성, 악성 가능성을 내포하고 있어 수술 시 음성 보전과 함께 종양학적 경계를 확보하는 것이 중요하다. 치료로는 cold instrument를 이용한 고식적 수술, CO 2 레이저를 이용하는 미세절제술, 혈관용해 레이저를 이용한 거상술 등이 시행되고 있다. CO 2 레이저를 이용한 수술적 방법은 절제술이 용이하다는 장점을 가져 현재까지 많이 시행되고 있으나 레이저에 의한 열손상으로 인해 정상 조직까지의 손상을 유발해 성대 협착(glottic stenosis), 성대 섬유화(vocal fold fibrosis), 피열연골 고정(arytenoid fixation)을 유발할 수 있으며[ 11], 반복적인 수술 시에는 음성의 질을 낮출 수 있다는 점이 보고되었다[ 12]. 혈관용해 레이저는 붉은 빛의 물질을 선택적으로 흡수하여 혈관이 풍부한 조직에 광열분해를 일으키는 레이저들을 일컫는다. Potassium titanyl phosphate laser (KTP, 532 nm), pulsed dye laser (585-600 nm) 등이 후두수술에 적용되었으며, 우리나라에는 532 nm의 diode laser가 주로 이용되고 있다. 혈관용해 레이저는 상피하 미세혈관 구조(subepithelial microvasculature)에 광열분해를 일으켜 상피와 고유층의 표면의 분리를 야기하여 미세피판수술(microflap surgery) 하는데 강점을 가지며, 섬유화(fibrotic change)의 위험성이 적으며 굴곡 광섬유(flexible fiberoptics)를 사용하여 다양한 위치에서의 조사가 가능하다[ 13]. 혈관용해 레이저는 특히 혈관성 병변(재발성후두유두종, 혈관성폴립 등)과 재발성 표재성 성대점막질환(백반증, 성대구증 등)에 유용한 술식으로 보고되고 있다. 아울러 다양한 술식 변형이 가능하여 조기성문암과 같은 악성 병변에서도 활용이 가능하나 넓은 범위의 병변을 제거할 시에는 상대적으로 시간이 더 많이 소요될 수 있다는 단점이 있다[ 13]. 본 연구는 혈관용해 레이저를 통한 성대 점막 거상술이 음성 회복에 유의미한 결과를 보여주었으며 이를 통해 정상 조직의 최대 보존과 병변의 완전 절제를 가능하게 하는 치료법에 대해 제시하였다. 성대 진동의 평가는 음성의 평가에 있어서 필수적인 요소이며 사용의 편리함과 경제성으로 인해 비디오 스트로보스코피가 많이 사용되고 있다. 다만 스트로보스코피는 성대의 진동주기와 맞춰야만 점막파동의 의미 있는 촬영을 할 수 있어 불규칙한 성대의 움직임을 보이는 병변의 촬영에는 적합하지 않은 면이 있다. 이에 초당 2000장의 촬영을 하는 고속 후두촬영법이 사용되기도 하였으나, 이는 많은 양의 저장공간을 필요로 하며 즉각적인 피드백이 어렵다는 단점을 가지고 있었다. 2D DKG는 고속후두촬영법을 사용한 데이터를 한 장의 이미지로 정리하여 작은 저장공간을 차지하며 음성의 정량적 평가를 가능케 한다는 점에서 새로운 음성학적 평가 방법으로 대두되고 있다. 성대 백반증은 임상학적 정도에 따라 점막의 운동성이 감소 혹은 소실되어 있어 주관적인 분석에 기반을 두고 있는 기존의 스트로보스코피만으로는 정확한 측정의 한계를 갖는 경우가 있어 협대역 영상(narrow band imaging)의 사용을 요하기도 한다[ 14]. 2D DKG는 이와는 달리 고속촬영을 이용하여 정확한 시각화가 가능하며 객관적인 지표를 활용하여 성대의 진동에 대한 정량적 평가를 할 수 있다는 점에서 성대 백반증의 진단 및 평가에 차별화된 유용성을 지니고 있는 도구로 사용될 수 있음을 본 연구는 제시하고 있다. 본 연구는 2D DKG가 성대 백반증의 진단적 유용성을 평가하기 위해 ASI, PSI, OQ를 측정하여 이를 7점 척도의 GRBAS, ADSV의 켑스트럼 관련 변수, MDVP의 주기성 관련 음향학적 측정치, EGG 관련 변수, KVHI와 K-VFI의 설문 점수와 비교하였으며 수술 전후의 2D DKG의 척도 및 음성 척도 비교를 통해서 성대 거상술의 유용성을 확인하였다. 수술 전후의 2D DKG의 ASI의 감소 및 GRBAS 중 grade와 breathiness의 감소를 확인하였으며 ASI와 GRBAS의 grade와 breathiness가 서로 유의미한 상관관계를 보임을 확인하였다. 본 연구에서 혈관 분해성 레이저를 이용한 성대점막 거상술은 음성의 보존에 있어 유의미한 결과를 나타냈으며 환자의 주관적 증상과 2D DKG에서의 정량적 측정이 유효함을 확인할 수 있어 2D DKG의 진단적 도구로서의 유용성을 입증하였다. 또한 KVHI에서의 신체점수와 K-VFI에서의 피로감 점수의 수술 전후 비교 시 감소하여 혈관용해 레이저를 통한 성대 거상술이 성대 백반증에 대한 효과적인 수술적 치료임을 다시 한번 확인해 볼 수 있었다.
본 연구를 통해 성대 백반증의 수술적 치료방법으로서 혈관용해 레이저를 이용한 거상술이 음성 보존에 있어 효과적인 방법이며 2D DKG가 진단적 방법으로써 유효함을 보였다. 그러나 7명이라는 소규모 환자의 후향적 연구이며, 각 대상자의 술후 검사 시기의 범위가 다소 넓었다. 또한 수술적 방법의 대조군이 존재하지 않아 수술적 방법의 가능성을 제시할 수는 있으나 타 수술방법과의 비교 우위를 확인할 수 없었다는 점에서 한계가 있으므로 후속 연구에서는 이를 보완하여야 한다. 마지막으로 2D DKG는 기존의 음성검사 지표들과 연관성을 일부에서만 나타내고 있어, 음성의 개선 정도에 대한 추가적인 검사방법 및 정량 지표를 이용한 보다 대규모의 후속 연구가 필요하다고 판단된다.
ACKNOWLEDGMENTS
This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number: 1711174497, RS-2020-KD000093). This work was also supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2021R1G1A1094247).
Fig. 1.
The surgical procedures of angiolytic laser stripping for vocal fold leukoplakia. A: Stroboscopic finding before surgery. B: The tip of the flexible laser fiber was grasped using alligator forceps and moved to its target within 3 mm of the lesion. C: After irradiating the entire lesion, the leukoplakic epithelium was separated and elevated from the vocal folds using a small cotton ball and grasping forceps. D: Surgical field after angiolytic laser stripping. 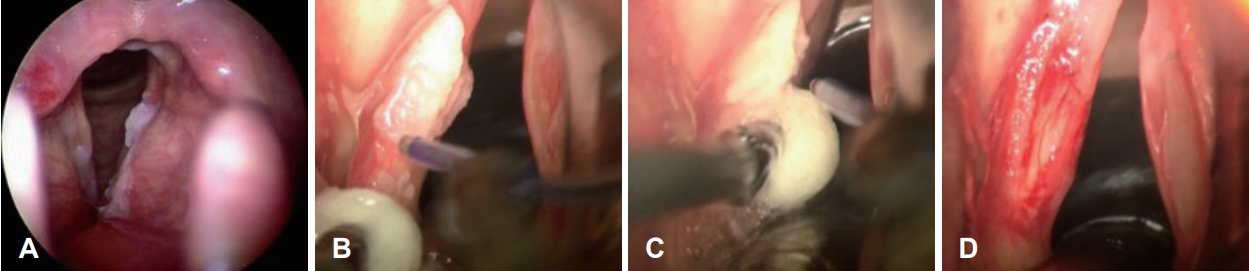
Fig. 2.
Parameters of vocal fold vibratory characteristics using the 2D scanning digital kymography. Amplitude symmetry index=(AR-AL)/(AR+AL), phase symmetry index=(TR+TL)/T, open quotient=TO/T. Normophonic male (67 years old). 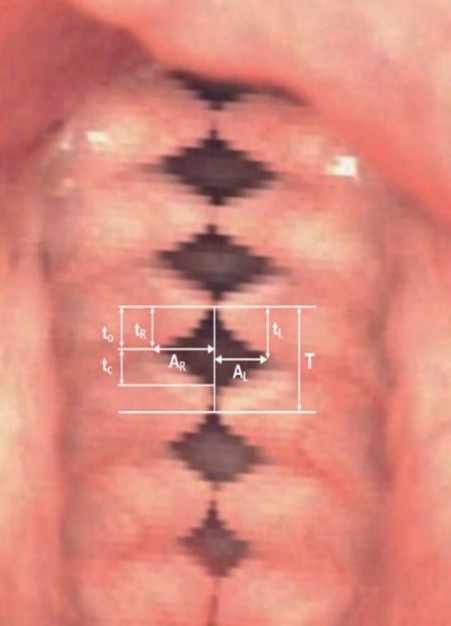
Fig. 3.
Pre- and post-operative findings of the lesion sites and post-operative 2D DKG finding for each case are presented in the top, middle, and bottom line, respectively. 2D DKG, two-dimensional scanning digital kymography. 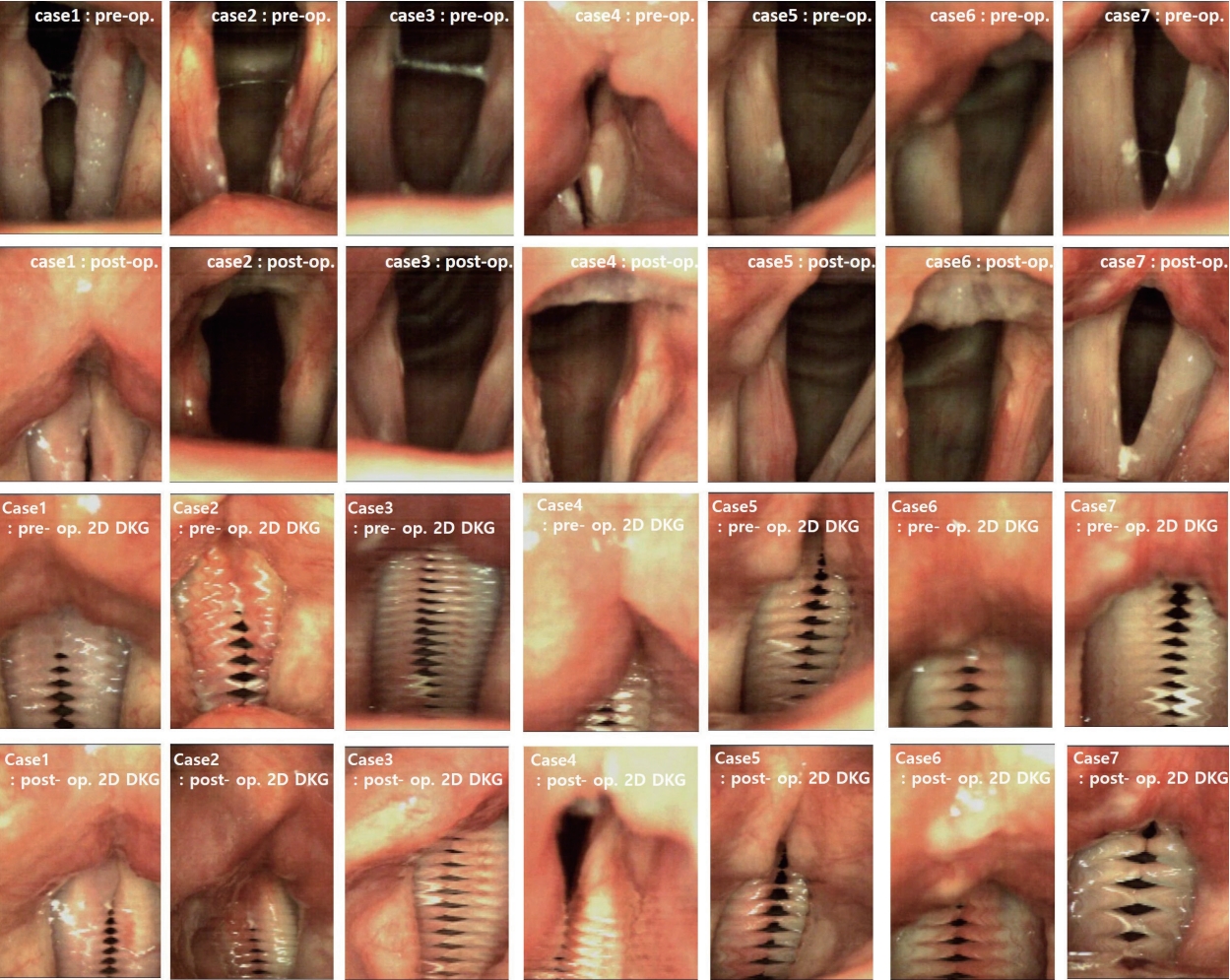
Fig. 4.
Correlation between the changes in the 2D DKG parameters and voice outcomes after angiolytic laser stripping for unilateral vocal fold leukoplakia. ASI, amplitude symmetry index; KVHI, Korean version of Voice Handicap Index; K-VFI, Korean version of Vocal Fatigue Index; OQ, open quotient; 2D DKG, two-dimensional scanning digital kymography. 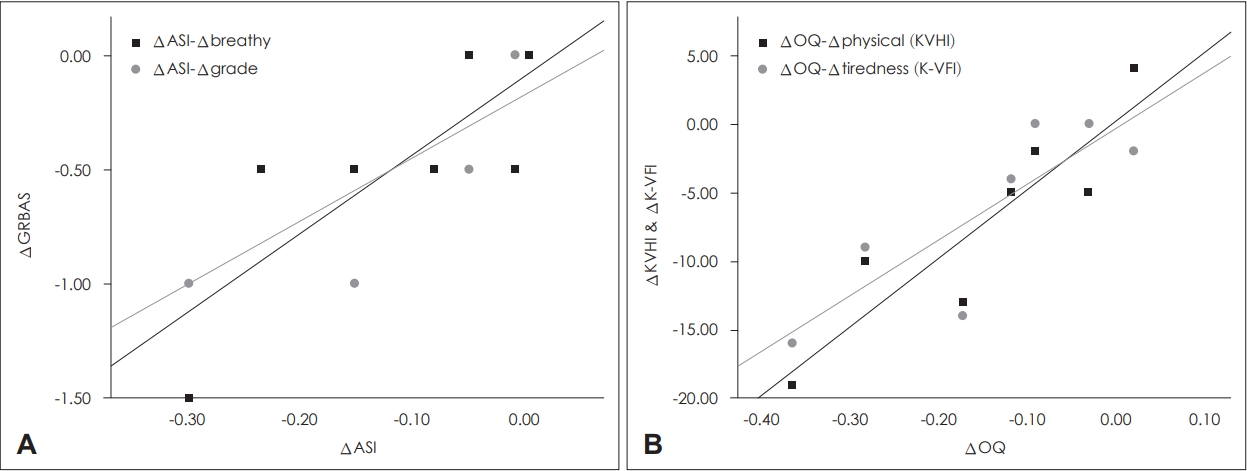
Table 1.
Demographic and clinical characteristics of the patient population (n=7)
|
Characteristic |
Value |
|
Age (year) |
62.14 (39-74) |
|
Sex |
|
|
Male |
7 (100) |
|
Female |
0 (0) |
|
Site |
|
|
Left |
3 (42.9) |
|
Right |
3 (42.9) |
|
Both |
1 (14.2) |
|
Pathology |
|
|
Hyperkeratosis |
6 (85.8) |
|
Dysplasia (low grade) |
1 (14.2) |
|
Laser pulse delivered |
|
|
Irradiance, Watt/cm2
|
4.3±0.5 |
|
Fluence, Joules/cm2
|
83.5±27.4 |
|
Follow-up period (day) |
82.57±28.55 |
Table 2.
Comparative analysis of pre- and post-operative variables
|
Pre-op |
Post-op |
p-value |
|
2D DKG |
|
|
|
|
ASI*
|
0.17±0.12 |
0.08±0.07 |
0.028*
|
|
PSI |
0.08±0.07 |
0.05±0.43 |
0.866 |
|
OQ |
0.71±0.12 |
0.56±0.83 |
0.028*
|
|
GRBAS |
|
|
|
|
G |
2.10±0.53 |
1.57±0.53 |
0.038*
|
|
R |
1.86±0.70 |
1.43±0.73 |
0.059 |
|
B |
1.64±0.38 |
1.14±0.48 |
0.034*
|
|
A |
0.00±0.00 |
0.00±0.00 |
>0.999 |
|
S |
1.57±0.45 |
1.36±0.63 |
0.083 |
|
ADSV |
|
|
|
|
CPP |
12.488±3.660 |
11.473±3.559 |
0.063 |
|
σCPP |
0.905±0.608 |
0.849±0.191 |
>0.999 |
|
SR |
34.610±5.858 |
32.441±7.164 |
0.176 |
|
σSR |
1.501±0.549 |
1.479±0.225 |
0.866 |
|
MDVP |
|
|
|
|
Jitt |
1.147±1.211 |
1.661±2.083 |
0.237 |
|
Shim |
4.660±2.794 |
5.510±3.525 |
0.176 |
|
NHR |
0.150±0.037 |
0.161±0.069 |
0.866 |
|
EGG |
|
|
|
|
SFF |
127.19±18.42 |
121.04±17.24 |
0.176 |
|
σSFF*
|
18.16±6.13 |
15.29±3.27 |
0.043*
|
|
CQ |
43.92±2.83 |
45.15±3.76 |
0.398 |
|
σCQ |
5.49±3.18 |
4.88±1.30 |
0.735 |
|
VHI |
|
|
|
|
VHI-TTL |
35.7±14.5 |
20±24.0 |
0.075 |
|
Functional |
11.1±4.7 |
6.9±8.2 |
0.128 |
|
Physical*
|
15.4±6.6 |
8.3±9.9 |
0.042*
|
|
Emotional |
9.1±5.0 |
4.9±6.4 |
0.058 |
|
VFI |
|
|
|
|
VFI-TTL*
|
27.1±10.1 |
16.4±14.9 |
0.043*
|
|
Tiredness*
|
15.1±6.0 |
8.7±9.1 |
0.043*
|
|
Physical |
15.4±6.6 |
2.9±3.8 |
0.058 |
|
Rest |
6.6±2.5 |
4.9±5.4 |
0.173 |
REFERENCES
3. Yamauchi A, Yokonishi H, Imagawa H, Sakakibara K, Nito T, Tayama N, et al. Quantification of vocal fold vibration in various laryngeal disorders using high-speed digital imaging. J Voice 2016;30(2):205-14.   4. Bae IH, Park HJ. Automated quantitative analysis of vocal fold vibration using two-dimensional scanning videokymography after transoral laser microsurgery. Clin Arch Commun Disord 2021;6(1):39-47.  5. Kang DH, Wang SG, Park HJ, Lee JC, Jeon GR, Choi IS, et al. Realtime simultaneous DKG and 2D DKG using high-speed digital camera. J Voice 2017;31(2):247.e1-7. 6. Bae IH, Wang SG, Lee JC, Sung ES, Kim ST, Lee YW, et al. Efficacy of two-dimensional scanning digital kymography in evaluation of atrophic vocal folds. J Voice 2019;33(4):554-60. 7. Kim GH, Lee YW, Bae IH, Park HJ, Wang SG, Kwon SB. Usefulness of two-dimensional digital kymography in patients with vocal fold scarring. J Voice 2019;33(6):906-14. 8. Choi SH, Yu M, Choi CH. Comparisons of 4-point GRBAS, 7-pointGRBAS, and CAPE-V for auditory perceptual evaluation of dysphonia. Audiol Speech Res 2021;17(2):206-19. 9. Kim JO, Lim SE, Park SY, Choi SH, Choi JN, Choi HS. Validity and reliability of Korean-version of voice handicap index and voicerelated quality of life. Speech Sciences 2007;14(3):111-25.
10. Kim MJ. Relationship between vocal fatigue index and voice handicap index for professional voice users [dissertation]. Seoul, Ewha Womans Univ.; 2017.
11. Siegel B, Smith LP. Management of complex glottic stenosis in children with recurrent respiratory papillomatosis. Int J Pediatr Otorhinolaryngol 2013;77(10):1729-33. 13. Kang MS, Lim JY. Update on angiolytic laser laryngeal surgery. J Korean Soc Laryngol Phoniatr Logop 2021;32(2):51-5.
|
|














