Introduction
Humans generally spend one-third of their life sleeping. Sleep is an active, comprehensive physiological process that has a crucial impact on health and daytime functioning [1]. Obstructive sleep apnea (OSA) syndrome is defined by repetitive pauses in breathing during sleep, despite the effort to breathe in the presence of at least five episodes of obstructive apnea and/or hypopnea per hour of sleep with associated symptom. During sleep, OSA patients repeatedly attempt inspiration but fail because of upper airway obstruction. OSA is associated with day time sleepiness, hypertension, depression, insulin resistance, metabolic syndrome, subsequent cardiac ischemia, and arrhythmias [2,3].
Recently, several studies have shown that right lateral sleep position (RLSP) or left lateral sleep position (LLSP) may have different effects on sleep apnea in OSA patients [4,5]. Ozeke, et al. [4] reported that LLSP was associated with worse position-specific apnea-hypopnea index (AHI) compared with RLSP. However, scientific evidence is still scarce and no study has investigated the possible factors that can influence the positional difference of OSA severity, including anthropometric or anatomic factors.
Until now, however, there has been no consideration for the discordance of both nasal cavity dimensions on the difference of AHI when evaluating both lateral sleeping positions. Although Leitzen, et al. [6] reported that abnormal nasal anatomy was not significantly correlated with OSA severity, they analyzed unquantified parameters such as turbinate hypertrophy, septal deviation, and internal nasal valve status using anterior rhinoscopy.
Based on the result of the above studies, we hypothesized that the difference in nasal cavity size could affect the sleep position and severity of sleep apnea. Thus, the present study was undertaken to evaluate the effect of sleep position and nasal cavity dimension according to minimal cross-sectional area (MCA) using acoustic rhinometry (AR) on OSA severity.
Subjects and Methods
Participants
A retrospective review of data was performed in a tertiary hospital. The study was approved by the Institutional Ethics Committee of Korea University Ansan Hospital (2018AS0277). We examined 623 records of all snoring patients who successfully completed overnight polysomnography (PSG) and recorded the duration of sleep position simultaneously from June 2012 through Jan 2019. Ninety-five patients were excluded from the study if they had evidence of impaired cardiac function, chronic obstructive pulmonary disease, history of previous nasal operation, and history of other nasal pathology including polyp, mass, and sinusitis, or incomplete data. Finally, 528 patients were enrolled in this study for evaluation of the assessment of OSA severity, body mass index (BMI), and upper airway anatomy according to lateral sleep posture. When we evaluated the association between sleep position and AHI value, we only included the patient who spent at least 20 minutes at each posture (RLSP or LLSP) during sleep, because too little sleep time in each position would impair the reliability of AHI data. With this process, 328 patients were excluded for evaluation of association between sleep position and OSA severity according to AHI value. Demographic and comorbidity data of the participants, including age, gender, and BMI were obtained. The patients also received a full otorhinolaryngology evaluation to address anatomical variations including nose, oral cavity and oropharynx, and anthropometric evaluations. Modified Mallampati score (MMS) and tonsillar grade were evaluated according to the FriedmanŌĆÖs classification [7].
Polysomnographic evaluation
Participants underwent overnight PSG using an Alice3 device (Healthdyne Technologies Inc., Marietta, GA, USA) to monitor the electroencephalogram (C3-A2, C4-A1), left and right electro-oculograms, electrocardiogram, chin and anterior tibialis electromyograms, abdominal and thoracic movements by piezoelectric bands, nasal and oral airflow, and oxygen saturation by pulse oximetry (SpO2). Obstructive apnea was defined as a reduction in airflow >90% lasting Ōēź10 s, during which time there was evidence of persistent respiratory effort. Hypopneas were defined as a decrease in nasal airflow of Ōēź30% with a corresponding decrease in SpO2 Ōēź4% for longer than 10 seconds. The sleep architecture was scored in 30-seconds epochs, and the sleep stage was interpreted according to standard criteria. The polysomnographic data were manually scored by well-trained sleep technicians and reviewed by certified sleep physicians in accordance with the recommended rule in American Academy of Sleep Medicine criteria [8]. In addition to routine polysomnographic data, position-specific sleep time and AHI were also acquired.
AR
In order to quantitatively measure the nasal cavity dimension, AR was performed at the initial visit using a previously described method by our institution without decongestion of nasal mucosa [9]. The AR study was performed in a quiet room with a door closed and data were obtained by using a twomicrophone acoustic rhinometer (Hood Laboratories, Pembroke, MA, USA). The free end of the nosepiece was fitted tightly to the anterior nares without deformation of the nasal vestibule. The patients were asked to hold a short breath and not swallow during measurement. The results were taken from the AR Eccovision computerized data program (Hood Laboratories) and were entered into a spreadsheet before calculation. We obtained the MCA value, which was defined as the narrowest cross-sectional area in the nasal cavity, usually represent the anterior end of the inferior turbinate. According to the MCA value between both nasal cavities, we divided the patient into two groups, the wide lateral side sleep position (WLSP) and narrow lateral side sleep position (NLSP). Patients who spent more time sleeping in the direction of the nasal cavity of the larger MCA value was included in the WLSP group, while those who dominantly slept in the direction of the smaller MCA value was included in the NLSP group. When comparing the size of nasal cavity dimensions, cases with exactly same MCA values were considered identical, and any slight differences in the dimensions were noted.
Statistical analysis
The SPSS statistical software package (version 13.0; SPSS Inc., Chicago, IL, USA) was used to perform all statistical calculations. Sleep time and AHI on each sleep posture were compared via paired-t test for normally distributed data and Wilcoxon signed rank test for that which did not follow a normal distribution. Then, subgroup analysis of sleep time and AHI at each position were also performed according to the presence of obesity according to WHO guideline for the Asia-Pacific perspective (BMI <23, 23-27.5 and Ōēź27.5 kg/m2), OSA severity, tonsil grades, or MMS [7,10]. The chi-square test was also performed for evaluation of the percentage of patients according to nasal cavity dimension in the RLSP and LLSP dominant groups. For all tests, a value of p<0.05 was considered statistically significant.
Results
Five-hundred and twenty-eight patients (470 males, 58 females) were enrolled. The mean age was 44.57┬▒13.04 years and mean BMI was 26.56┬▒4.10 kg/m2. In polysomnographic finding, the mean AHI was 31.61┬▒25.99/hour and composed of 73 (13.82%) simple snorers, 101 (19.13%) mild OSA, 135 (25.57%) moderate OSA, and 176 (33.33%) severe OSA patients. Additional baseline characteristics of the study population are shown in Table 1.
Assessment of positional sleep time and AHI according to WLSP and NLSP
The NLSP-specific sleep time was longer than that of WLSP (20.46%┬▒19.54% for NLSP and 16.00%┬▒16.44% for WLSP) with a statistically significant difference (p=0.001). When the patients were classified according to OSA severity, significant differences were found in mild and severe OSA patients (22.74%┬▒17.78% for NLSP vs. 15.77%┬▒16.59% for WLSP; p=0.001 and 19.39%┬▒18.76% for NLSP vs. 14.17%┬▒16.18% for WLSP; p=0.008, respectively). When the patients were classified according to BMI, the patients who were not overweight (BMI <23 kg/m2) did not show significant difference between RLSP and LLSP. Regardless of tonsil size and MMS, the sleep time of NLSP was longer than that of WLSP. Thus, tonsil grade and MMS did not have an effect of the difference of positional sleep time according to nasal cavity dimension (Table 2).
We also evaluated the positional AHI between WLSP and NLSP groups. However, no significant difference of AHI was found between the two groups in all patients, and after classification according to BMI, tonsil grade, and MMS (Table 3).
Assessment of positional sleep time and AHI according to RLSP and LLSP
The positional sleep time for each sleep position were 257.40┬▒107.13 minutes (64.42%) on SSP, 82.00┬▒75.53 minutes (20.52%) on RLSP, and 60.19┬▒61.65 minutes (15.06%) on LLSP. The RLSP-specific sleep time was longer than that of LLSP with a statistically significant difference (p<0.001). When the patients were classified according to OSA severity, significant differences were found in moderate to severe OSA patients (23.76%┬▒21.65% for RLSP vs. 16.71%┬▒17.36% for LLSP; p=0.016 and 19.53%┬▒19.38% for RLSP vs. 14.02%┬▒ 15.31% for LLSP; p=0.004, respectively). Patients who were not overweight (BMI <23 kg/m2) or who have large tonsils did not show significant difference between RLSP and LLSP (Table 4). However, RLSP was longer than that of LLSP regardless of MMS.
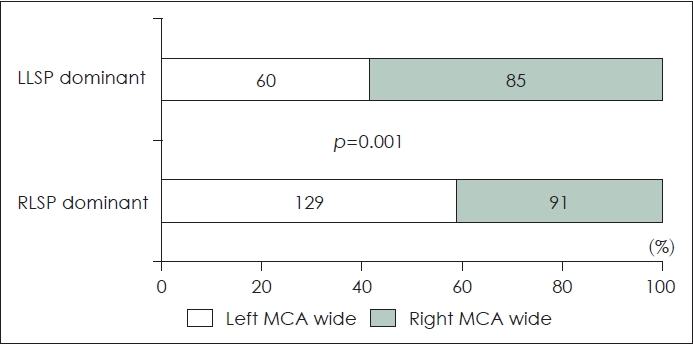
We also evaluated the percentage of patients according to nasal cavity dimension in RLSP and LLSP-dominant patients. In the RLSP dominant group, the number of left nasal cavity narrowed patients were fewer than that of right nasal cavity narrowed patients (91 vs. 129, respectively). In the LLSP dominant group, the number of right nasal cavity narrowed patients were fewer than that of left nasal cavity narrowed patients (60 vs. 85, respectively, p=0.001) (Fig. 1). This result show that, regardless of the right or left sleep position, people tend to sleep lying on the narrow side of nasal cavity (129/220 [58.64%] in RLSP dominant group, 85/145 [58.62%] in LLSP dominant group).
The positional AHI for RLSP was not statistically different from that of LLSP (17.24┬▒22.94 vs. 16.89┬▒23.61; p=0.528) in all patients. In addition, no statistical differences were found between RLSP and LLSP, even when the patients were classified according to the severity of OSA, BMI, tonsil grade, and MMS (Table 5).
Discussion
This study shows the sleep time in snoring patients was longer on RLSP compared with LLSP. Furthermore, we also found that the sleep time was longer in NLSP than WLSP. However, the AHI value was not significantly different according to sleep position.
The influence of sleep position (supine vs. lateral sleep position) on OSA has been evaluated in several studies [11-13]. Even though the definition of positional treatment differed among the various studies, more than half of the OSA patients displayed a Ōēź50% difference in the apnea index between the supine and lateral positions [14]. A review of positional treatment for OSA reported a positive effect of positional treatment on the AHI and the compliance of the positional treatment is better than full term for CPAP compliance [13]. The physiologic mechanism responsible for this positional effect on OSA is most probably related to the effect of gravity on the upper airway. In the supine posture, gravitational forces increase the tendency of the tongue and soft palate to fall back into the throat, creating a smaller caliber upper airway. In this sleep position, the likelihood for the airway to become obstructed is higher, which would lead to the occurrence of a large number of sleep apnea episodes [14].
However, few studies have investigated the difference of RLSP and LLSP in OSA patients without significant cardiovascular comorbidities. Ozeke, et al. [4] reported that LLSP-specific AHI score was statistically higher than that for RLSP (30.2┬▒32.6/h vs. 23.6┬▒30.1/h; p<0.001). In the present study, a significant difference of RLSP and LLSP AHI was not evident. Furthermore, the OSA severity also did not influence the difference of positional AHI.
In this study, the sleep time was longer for RLSP than LLSP, especially in overweight patients. We do not know the exact mechanism by which BMI affects the difference of sleep time between RLSP and LLSP. However, LLSP interferes with the free action of the heart, increases sympathetic nervous activity, and facilitates the left-to-right shunting of blood and resultant hypoxemia in the case of patent foramen ovale compared to RLSP [4,15]. These changes may aggravate the breathing difficulty and hypoxemia while in the LLSP. BMI is closely related to the volume of lateral pharyngeal wall, including parapharyngeal fat [16]. A possible explanation that may provide some insight into this issue could be the association between airway obstruction pattern and the volume of the lateral pharyngeal wall. BMI and volume of lateral pharyngeal wall are the main determinants for positional dependence and may cause different patterns of airway obstruction during sleep or sleep-like conditions [16-20]. Patients who are obese or who have larger lateral pharyngeal wall volume have a greater chance of concentric type airway narrowing in drug-induced sleep endoscopy, which may increase the burden on the cardiopulmonary system and increase the activity of sympathetic nervous system. Thus, obese patients prefer RLSP in order to reduce this inconvenience. We also found that the durations of RLSP and LLSP were not significantly different in patients with large tonsils. There are no reports on the relationship between tonsil size and lateral sleep position, so we cannot explain the exact mechanism. Pevernagie and Shepard [21] reported that changing the posture from supine to lateral might affect the lateral diameter, but not the anteroposterior diameter of the upper airway at the level of the pharynx. Thus, we suggest that, the lateral diameter change of pharynx according to body position might be small in patients with large tonsils and has little impact on inconvenience during sleep.
In general, nasal anatomical abnormalities were not considered to have a significant effect on OSA pathophysiology [22]. However, Silvoniemi, et al. [23] reported that, severe nasal obstruction due to nasal septal deviation can lead to breathing disturbance during sleep. Furthermore, several studies reported that, correction of nasal anatomical deformity such as nasal septal deviation or nasal turbinate hypertrophy might have beneficial effects on sleep quality [24-26]. In this study, we found that the sleep time was longer for NLSP than WLSP regardless of the RLSP or LLSP predominance. According to nasal physiology, the nasal cavity volume of the dependent side is significantly reduced [27]. If the patient goes to sleep in the WLSP, the wide side nasal cavity becomes narrow, making it difficult to breathe due to nasal obstruction. Thus, the patient tends to sleep on the more comfortable side. However, we also did not find a significant difference of AHI between WLSP and NLSP. Therefore, we suggested that the difference in nasal cavity dimension did not affect the OSA severity according to AHI.
The present study has some limitations. First, AR was performed at first visit in sitting position without nasal decongestant use. Thus, nasal physiology, such as nasal cycle and patientŌĆÖs position, might affect the nasal cavity dimension and might not correlate with the situation during sleep. Furthermore, we did not evaluate the association of subjective nasal blockage and nasal cavity narrowness. Of course, it is more accurate to conduct the evaluation obtained by performing the test several times at various points during sleep with evaluation of subjective nasal obstruction, unfortunately this study was performed by the retrospective method, so performing additional tests or questionnaires was not possible. Second, we only included patients who spent at least 20 minutes at each posture for evaluating the association between sleep position and AHI. In this step, about 60 percentages of patients were excluded finally. Thus, our findings might reflect some selection bias. However, several previous studies evaluated only the AHI values of patients who have been sleeping for more than 20 or 30 minutes at a lateral position [28-30]. Therefore, as mentioned above, we also considered that too little sleep time in each position would impair the reliability of AHI data. In conslusion, the snoring patients preferred RLSP compared with LLSP, and prefer sleep on the lateral side of the narrow nasal cavity. The OSA severity was not significantly different according to sleep position and nasal cavity dimension.