Introduction
Sudden sensorineural hearing loss (SSNHL) is defined as a hearing loss of 30 dB or more over at least three consecutive audiometric frequencies occurring within a 72-hour period [1]. Although idiopathic cause is most common, several studies have hypothesized a relationship between viral infection and SSNHL [2]. The virus species included herpes simplex virus (HSV), human immunodeficiency virus (HIV), measles, rubella, mumps, and so on [2]. In addition, the aural symptoms of HIV infection include otalgia, vertigo, tinnitus, otorrhea, and hearing loss [3]. Various mechanisms of auditory dysfunction in HIV/acquired immune deficiency syndrome (AIDS) have been proposed [3]. These also include opportunistic infections associated with hearing loss and ototoxicity due to highly active antiretroviral treatment, as well as medications used to treat opportunistic infections [3]. In this case, we report a patient with HIV infection with associated sequential bilateral SSNHL and acute otitis media (AOM) on the left side. A 35-year-old male, who had never previously been diagnosed with HIV infection, presented with abrupt otologic symptoms. Serum anti-HIV antibodies were subsequently detected. Although the relationship between HIV virus and sudden hearing loss has been proposed in previous studies, the case in which the initial presentation of HIV infection is SSNHL and unilateral AOM is rare. That is the why we report this case.
Case
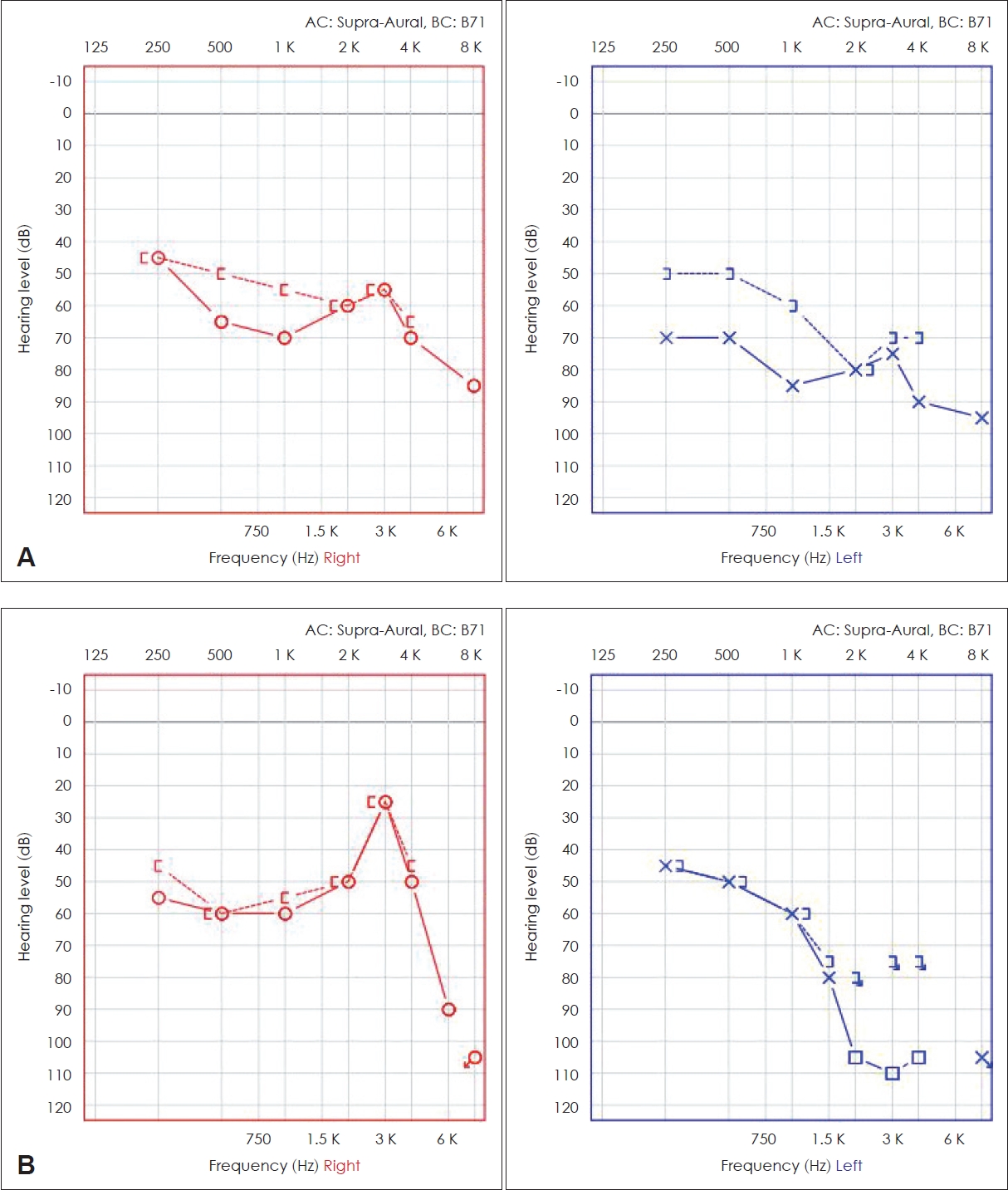
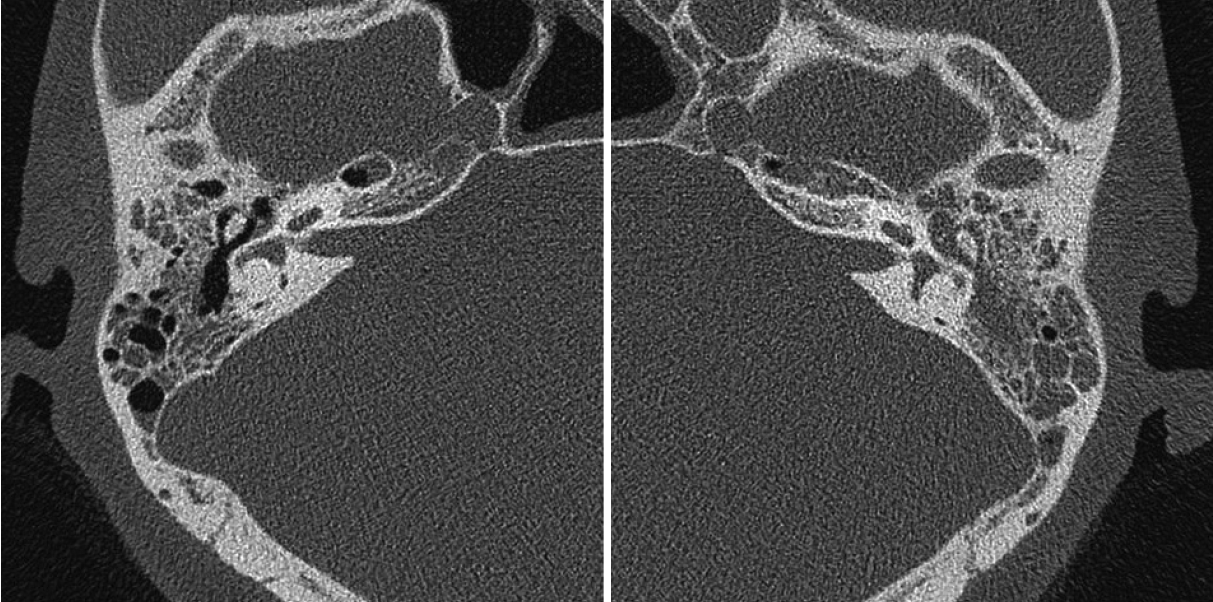
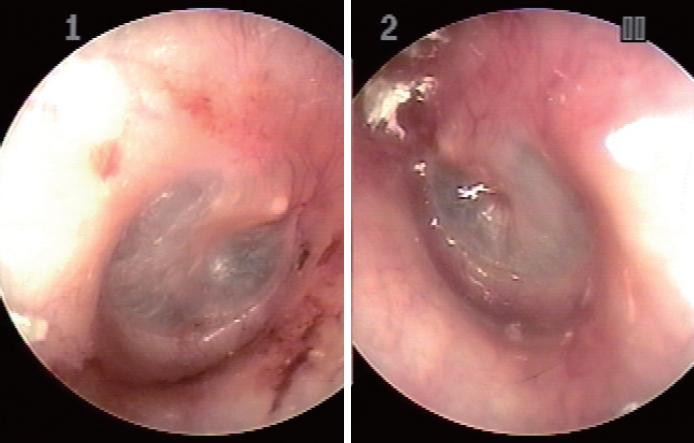
A 35-year-old male visited our hospital because of sudden hearing loss on both sides, left otalgia, and left otorrhea. His previous hearing was normal and he did not complain of dizziness or neurological abnormalities and right side otalgia. Eight days prior, sudden hearing loss had developed in the right ear as a first symptom; two days later, sudden hearing loss in the left ear with otalgia also appeared. On otoscopic examination, the patient presented with no abnormalities in the right ear. In the left ear, mild redness, bulging of the tympanic membrane, and serous otorrhea were observed. Audiometry revealed both mixed type hearing loss (Fig. 1A) but tympanometry (Fig. 2) was type As in the both side ear. The patient had no trauma, surgical history, and no underlying disease. Temporal bone CT revealed focal soft tissue density in the right middle ear cavity and near total soft tissue opacification in the left middle ear and mastoid cavity (Fig. 3). Temporal MRI revealed diffuse T2 hyperintensity in both middle ear and mastoid cavity and no other remarkable abnormalities.
The left side otalgia, otoscopic finding of bulging and injection of the eardrum and CT finding of middle ear cavity soft tissue density suggest that AOM was accompanied in the left ear. However, the right ear has no otalgia, injection and bulging of the eardrum, and the middle ear cavity was relatively clean on CT. In addition, left side SSNHL cannot be excluded because it was not accompanied by dizziness, the air bone gap of PTA was small, and bone conduction threshold didnвАЩt change before and after treatment. Therefore, the cause of hearing loss in the left ear are both likely to be SSNHL and SNHL from AOM.
In conclusion, he was diagnosed with SSNHL on both sides and AOM on the left side. Subsequently, corticosteroid therapy (intratympanic injection dexamethasone 4 times, intramuscular injection prednisolone 6 days 187.5 mg, 187.5 mg, 125 mg, 125 mg, 75 mg, 75 mg), and antibiotics (IV ceftriaxone IV, IV amikacin 10 days) was administered. The patient underwent a series of serological tests (syphilis, HSV, herpes zoster, toxoplasmosis, measles, hepatitis A virus; hepatitis B virus; hepatitis C virus) and tested positive for HIV antibodies. The others tested negative. He had no symptoms such as fever or respiratory symptoms and had never previously been diagnosed with HIV. At the time of diagnosis, the HIV ribonucleic acid copy number of the patient was 7460 copies/mL and the CD4 lymphocyte count was 175 cells/mL. The patient was followed-up in the outpatient clinic two weeks after discharge, and redness, swelling of the left eardrum, and otalgia improved (Fig. 4). However, hearing did not improve significantly. The patient maintained HIV treatment (antiviral drug: Efavirenz, lamivudine, zidovudine) and was undergoing yearly follow-up in an outpatient clinic. After 2 years, his right hearing improved, but it had plateaued without further improvement on both sides (Fig. 1B). There was no other additional symptoms.
Discussion
Hearing loss associated with AIDS can be caused by a central nervous system neoplasm, as a secondary effect of iatrogenic causes after ototoxic drug administration, as a direct result of HIV infection of the central nervous system or the peripheral auditory nerve, or as a result of another infection (viral or bacterial infection) [4]. According to Lin, et al. [4], on patients aged 18 to 35 years, HIV infection is significantly associated with an increased risk of developing SSNHL, with an adjusted hazard ratio of 2.169 (p<0.05). Schouten, et al. [5] and Onen, et al. [6] mentioned HIV causes the acceleration of patientsвАЩ biological aging. According to Schouten, et al. [5], compared to HIV-uninfected controls, individuals with HIV infection were statistically more likely to have all age-associated non-communicable comorbidities, peripheral artery disease, cardiovascular disease, and impaired renal function. Onen, et al. [6] compared the incidence of non-AIDS diseases in older people with HIV and the general population and found that HIV accelerates biological aging. Cranial nerve involvement in HIV infection may occur, most commonly in the 7th cranial nerve, while both side 8th cranial nerve involvement is rarely reported [7-9]. In this case, it appeared that HIV infection affected the 8th cranial nerve on both sides. This case is meaningful as it is the first reported case of HIV infection found with involvement of the 8th cranial nerve presenting as the initial symptom, in the absence of any other symptoms caused by HIV infection. AOM causes conductive hearing loss during the acute stage; however, recent research has also shown that patients with a history of acute or recurrent AOM have sensorineural hearing loss, particularly at high frequencies (2-8 kHz) [10]; conductive deficits in the acute phase are primarily caused by middle ear fluid, and the sensorineural component most likely results from intracochlear inflammation caused by the migration of inflammatory and toxic substances from the middle to inner ear through the round window membrane [10]. The patient in this case presented with bilateral mixed-type hearing loss. The right ear has no otalgia, injection and bulging of the eardrum, and the right middle ear cavity was relatively clean on CT. Therefore, he was diagnosed with SSNHL on right side. Although he had AOM on left ear, left side SSNHL cannot be excluded because it was not accompanied by dizziness, the air bone gap of PTA was small, and bone conduction threshold also didnвАЩt change before and after treatment. Therefore, the cause of hearing loss in the left ear are both likely to be SSNHL and SNHL from AOM.
In conclusion, a 35-year-old male was diagnosed with sudden bilateral hearing loss and acute otitis on the left side, and subsequent serological examination revealed HIV infection. The cases reported so far have involved patients who had been previously diagnosed with HIV infection in whom bilateral hearing loss involving the 8th cranial nerve was later identified. This case is meaningful as it is a case of HIV infection diagnosed after the identification of the invasion of the 8th cranial nerve as the first symptom, in the absence of any other HIV infection-associated symptoms.