ņä£ ļĪĀ
ņĀäņØīņä▒ ļé£ņ▓ŁņØĆ ņÖĖņØ┤, Ļ│Āļ¦ē, ņżæņØ┤Ļ░ĢņØś ļ¼ĖņĀ£ļĪ£ ĻĖ░ļÅäļź╝ ĒåĄĒĢ£ ņåīļ”¼ņØś ņĀäļŗ¼ņØ┤ ņĀĢņāüņĀüņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņ¦Ćņ¦Ć ņĢŖņĢä ļ░£ņāØĒĢśļŖö ļé£ņ▓Łņ£╝ļĪ£ ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ņ£Āļ░£ĒĢśĻ▓ī ļÉśĻ│Ā ĻĘĖ ņĀĢļÅäļŖö ņøÉņØĖņØś ņ£äņ╣śņŚÉ ļö░ļØ╝ ļŗżļźĖļŹ░ 20-25 dB ņØ┤ņāüņØś ĻĖ░ļÅäĻ│©ļÅäņ░©ļŖö ņżæņØ┤ņØś ļ¼ĖņĀ£ļź╝ ņÜ░ņäĀņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢśļ®░, ņł£ņłśĒĢ£ ņĀäņØīņä▒ ļé£ņ▓ŁņŚÉņä£ ĻĖ░ļÅäņ▓ŁļĀźņØĆ 60 dBņØä ņ┤łĻ│╝ĒĢśņ¦Ć ņĢŖļŖöļŗż[1-3]. Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØĆ ĻĖ░ļÅäņ▓ŁļĀźĻ│╝ Ļ│©ļÅäņ▓ŁļĀź ņŚŁņ╣śĻ░Ć ļ¬©ļæÉ ņ”ØĻ░ĆļÉśņ¢┤ ņ׳ņ£╝ļ®┤ņä£ ĻĖ░ļÅä ņ▓ŁļĀźņØ┤ 10 dB ņØ┤ņāü ļŹö ņ”ØĻ░ĆļÉ£ Ļ▓ĮņÜ░ļź╝ ņØśļ»ĖĒĢ£ļŗż[4]. ņÜ░ļ”¼ļéśļØ╝ ĻĄŁļ»╝Ļ▒┤Ļ░Ģņśüņ¢æņĪ░ņé¼(2010-2012) Ļ▓░Ļ│╝ņŚÉ ļö░ļź┤ļ®┤ 12ņäĖ ņØ┤ņāüņŚÉņä£ ņ£ĀĒśĢņŚÉ Ļ┤ĆĻ│äņŚåņØ┤ 25 dB ņØ┤ņāüņØś ļé£ņ▓ŁņØä Ļ░Ćņ¦ĆļŖö ļ╣äņ£©ņØĆ 22.73%ļĪ£ ņĪ░ņé¼ļÉśņŚłļŗż[5]. ņŗ¼ņé¼ĒÅēĻ░ĆņøÉ ņ×ÉļŻīņŚÉ ļö░ļź┤ļ®┤ 2021ļģäļÅäņŚÉ ļé£ņ▓Łņ£╝ļĪ£ ņ¦äļŻīļ░øņØĆ ĒÖśņ×É ņłśļŖö 212757ļ¬ģņØĖļŹ░ ĻĘĖņżæ ņĀäņØīņä▒ ļé£ņ▓ŁĻ│╝ Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØĆ Ļ░üĻ░ü 24945ļ¬ģ(11.7%)ņÖĆ 52631ļ¬ģ(24.7%)ņØĖ Ļ▓āņ£╝ļĪ£ ņĪ░ņé¼ļÉśņŚłļŗż[6]. ĒĢ┤ņÖĖņØś ļ¼ĖĒŚīņŚÉņä£ļŖö 18ņäĖ ņØ┤ņāüņŚÉņä£ 25 dB ņØ┤ņāüņØś ļé£ņ▓Ł ĒÖśņ×ÉņØś ļ╣äņ£©ņØĆ 16%-20%ņØ┤Ļ│Ā[7-9], ņØ┤ ņżæ ņĀäņØīņä▒ ļé£ņ▓ŁņØś ļ╣äņżæņØĆ 3%-10%ļź╝ ņ░©ņ¦ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[8,9].
ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ņ£Āļ░£ĒĢśļŖö ņøÉņØĖņ£╝ļĪ£ļŖö ņÖĖņØ┤ļÅäņŚ╝, ņÖĖņØ┤ļÅä ĒÅÉņāē ļō▒ ņÖĖņØ┤ļÅäņØś ļ¼ĖņĀ£ņÖĆ Ļ│Āļ¦ēņ▓£Ļ│Ą, ņé╝ņČ£ņä▒ ņżæņØ┤ņŚ╝, ļ¦īņä▒ ņżæņØ┤ņŚ╝, ņ¦äņŻ╝ņóģ ļō▒ ņżæņØ┤ņØś Ļ░ÉņŚ╝ņØ┤ļéś ņŚ╝ņ”ØņŚÉ ņØśĒĢ£ Ļ▓ĮņÜ░Ļ░Ć ĒØöĒĢśĻ│Ā ļō£ļ¼╝Ļ▓ī ļé┤ņØ┤ ņ¦łĒÖśņŚÉ ĻĖ░ņØĖĒĢśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ļŗż[2,10]. ņŚ╝ņ”ØņŚÉ ņØśĒĢ£ ņżæņØ┤ ņ¦łĒÖśņØś Ļ▓ĮņÜ░ ļīĆļČĆļČä ņØ┤ļé┤ņŗ£Ļ▓Į ļō▒ņ£╝ļĪ£ Ļ│Āļ¦ēņØś ņØ┤ņāü ļśÉļŖö Ļ│Āļ¦ē ļé┤ļČĆņØś ļ│æļ│ĆņØä Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳ņ£╝ļéś[2], ļō£ļ¼╝Ļ▓ī ņĀĢņāü Ļ│Āļ¦ēņ×äņŚÉļÅä ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ļ│┤ņØ┤ļŖö ņ▓ŁļĀźļÅäļź╝ ļéśĒāĆļé┤ļŖö Ļ▓ĮņÜ░Ļ░Ć ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ Ļ▓ĮņÜ░ ļæÉļČĆņÖĖņāüņØś ļ│æļĀźĻ│╝ ņ¢┤ņ¦Ćļ¤╝ņ”ØņØ┤ļéś ņ▓ŁĻ░üĻ│╝ļ»╝ ļō▒ ļÅÖļ░ś ņ”ØņāüņØä ĒÖĢņØĖĒĢ┤ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ ņØīņ░© Ļ▓Ćņé¼ ļō▒ņ£╝ļĪ£ ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ Ļ▓░Ļ│╝ļź╝ Ļ▓Ćņ”ØĒĢśĻ│Ā ņ×äĒö╝ļŹśņŖż ņ▓ŁļĀźĻ▓Ćņé¼ņÖĆ ĒåĄĻĖ░ ņØ┤Ļ▓Į(pneumatic otoscope) ļō▒ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņżæņØ┤Ļ░Ģ ļé┤ļČĆņŚÉ ņל ļ│┤ņØ┤ņ¦Ć ņĢŖļŖö ļ│æļ│ĆņØä ņ░ŠņĢäļ│┤ņĢäņĢ╝ ĒĢ£ļŗż[1]. ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅä Ļ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļé£ņ▓ŁņŚÉņä£ ņĖĪļæÉĻ│© CTļź╝ ĒåĄĒĢ┤ ņØ┤ņåīĻ│©ņØä ĒżĒĢ©ĒĢ£ ņżæņØ┤Ļ░Ģ, ņ£Āņ¢æļÅīĻĖ░, ļé┤ņØ┤ ļ░Å ņĀäņĀĢņłśļÅäĻ┤ĆņØś ņāüĒā£ļź╝ ĒÖĢņØĖĒĢśļŖö Ļ▓āņØĆ ĒĢäņłśņĀüņØĖ ņ¦äļŗ© Ļ│╝ņĀĢņØĖļŹ░ ņĖĪļæÉĻ│© CTņŚÉņä£ļÅä ļ│æļ│ĆņØä Ļ┤Ćņ░░ĒĢĀ ņłś ņŚåļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņŗ£ĒŚśņĀü Ļ│ĀņŗżĻ░£ļ░®ņłĀļĪ£ ĻĘĖ ņøÉņØĖņØä ņ░ŠņĢäļ│┤ļŖö ļ░®ļ▓ĢņØ┤ ņ£ĀņØ╝ĒĢ£ ļ░®ļ▓ĢņØ┤Ļ│Ā 20 dB ņØ┤ņāüņØś ņĀäņØīņä▒ ļé£ņ▓ŁņØ┤ ņ¦ĆņåŹļÉĀ ļĢī ņŗ£ĒŚśņĀü Ļ│Āņŗż Ļ░£ļ░®ņłĀņØś ņĀüņØæņ”ØņØ┤ ļÉ£ļŗż[11]. ņŗ£ĒŚśņĀü Ļ│Āņŗż Ļ░£ļ░®ņłĀņØś Ļ▓ĮņÜ░ ĻĖ░ļÅäĻ│©ļÅäņ░©ņØś ņĀĢļÅä, ĒÖśņ×ÉņØś ļéśņØ┤, ļ░śļīĆņĖĪ ņ▓ŁļĀź ņāüĒā£, ĒÖśņ×ÉņØś ņäĀĒśĖļÅä ļō▒ņØä ļ¬©ļæÉ Ļ│ĀļĀżĒĢśņŚ¼ Ļ▓░ņĀĢĒĢśĻ▓ī ļÉśļŖöļŹ░ ņłśņłĀņØä ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░ ĻĘĖ ņøÉņØĖņØĆ ļ»Ėņāüņ£╝ļĪ£ ļé©Ļ▓ī ļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż.
ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļé£ņ▓ŁņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļōżņØĆ ņłśņłĀ Ļ▓░Ļ│╝ņŚÉ ļīĆĒĢ£ ļČäņäØņØ┤ļéś ņØ┤Ļ▓ĮĒÖöņ”Ø ļō▒ ĒŖ╣ņĀĢ ņ¦łĒÖśņØ┤ ĻĄŁĒĢ£ļÉ£ ļČäņäØņØ┤ ņŻ╝ļź╝ ņØ┤ļŻ©Ļ│Ā ņ׳ļŗż[10,12-14]. ĻĘĖļ¤¼ļéś ņŗżņĀ£ ņ×äņāüĒÖśĻ▓ĮņŚÉņä£ļŖö ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć ņØ┤ņ£ĀļĪ£ ņłśņłĀņØä ļ░øņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄĻĖ░ ļĢīļ¼ĖņŚÉ ņłśņłĀņØä ļ░øņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉļōżļÅä ĒżĒĢ©ĒĢśņŚ¼ ĻĘĖļōżņØś ņ×äņāüņ¢æņāüņØä ļČäņäØĒĢ£ Ļ▓░Ļ│╝ļŖö ņŗżņĀ£ ĒÖśņ×É ņ¦äļŻīņŚÉ ņ£ĀņÜ®ĒĢ£ ņĀĢļ│┤ļź╝ ņĀ£Ļ│ĄĒĢĀ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļ│æļĀź ņ▓ŁņĘ© ļō▒ņ£╝ļĪ£ ĻĘĖ ņøÉņØĖņØä ļ╣äĻĄÉņĀü ņēĮĻ▓ī ņ░ŠņØä ņłś ņ׳ļŖö ņÖĖņāüņä▒ ņØ┤ņåīĻ│© ņåÉņāüņØĆ ņĀ£ņÖĖĒĢśĻ│Ā ņŗ£ĒŚśņĀü Ļ│ĀņŗżĻ░£ļ░®ņłĀņØä ĒĢśņ¦Ć ņĢŖĻ│ĀļŖö ĻĘĖ ņøÉņØĖņØä ņĀĢĒÖĢĒ׳ ļŗ©ņĀĢĒĢśĻĖ░ ņ¢┤ļĀżņÜ┤ Ļ▓ĮņÜ░ļ¦īņØä ļīĆņāüņ£╝ļĪ£ ĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ņØś ļ¬®ņĀüņØĆ ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļ¬©ļōĀ ĒÖśņ×ÉļōżņØä ļ╣äņÖĖņāüņä▒ ļé£ņ▓ŁņØś ņ×äņāüņ¢æņāü, ņĖĪļæÉĻ│© CT ņåīĻ▓¼, ņ▓ŁļĀźĻ▓Ćņé¼ Ļ▓░Ļ│╝, ņøÉņØĖ ņ¦łĒÖś ļō▒ņØä ļČäņäØĒĢśļŖö Ļ▓āņØ┤ļŗż.
ļīĆņāü ļ░Å ļ░®ļ▓Ģ
ņŚ░ĻĄ¼ ļīĆņāü
2014ļģä 1ņøöļČĆĒä░ 2022ļģä 11ņøöĻ╣īņ¦Ć ļģĖņøÉņØäņ¦ĆļīĆĒĢÖĻĄÉļ│æņøÉ ņØ┤ļ╣äņØĖĒøäĻ│╝ ņÖĖļלļĪ£ ļé┤ņøÉĒĢśņŚ¼ ņŗ£Ē¢ēĒĢ£ ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ņŚÉņä£ ņĀäņØīņä▒ ļé£ņ▓Ł ļśÉļŖö Ēś╝ĒĢ®ņä▒ ļé£ņ▓Ł ņ¦äļŗ©ņØä ļ░øņØĆ 66ļ¬ģ ņä▒ņØĖ ĒÖśņ×ÉļōżņØś ņØśļ¼┤ĻĖ░ļĪØĻ│╝ ņĖĪļæÉĻ│© CTļź╝ ļČäņäØĒĢśņśĆļŗż. ļČäņäØ ļīĆņāüņØĆ 18ņäĖ ņØ┤ņāüņØś ņä▒ņØĖņ£╝ļĪ£ņä£ ņ¢æņĖĪ Ļ│Āļ¦ē ņåīĻ▓¼ņØ┤ ņØ┤ļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņŚÉņä£ ņĀĢņāüņØ┤Ļ│Ā, ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ņØś ņŚ░ņåŹļÉ£ ļæÉ ņŻ╝Ēīīņłś ņØ┤ņāüņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░©Ļ░Ć 20 dB ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ļź╝ ĒżĒĢ©ņŗ£ņ╝░ļŗż. ņÖĖņØ┤ ĻĖ░ĒśĢņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, Ļ│Āļ¦ē ļé┤ ņé╝ņČ£ņĢĪņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, ļæÉĻ▓ĮļČĆ ņÖĖņāüņØ┤ļéś ņłśņłĀļĀźņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ļŖö ņĀ£ņÖĖĒĢśņśĆļŗż. 66ļ¬ģ ĒÖśņ×ÉņØś 77ĻĘĆĻ░Ć ĒżĒĢ©ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśņŚ¼ ļČäņäØļīĆņāüņØ┤ ļÉśņŚłĻ│Ā ņĄ£ņóģ ņ¦äļŗ©ņØĆ ņłśņłĀņØä ĒåĄĒĢ┤ ĒÖĢņØĖļÉ£ ļ░öļ¦ī ĻĖ░ņ×¼ĒĢśņśĆĻ│Ā ņłśņłĀņØä ļ░øņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░ ļ»Ėņāüņ£╝ļĪ£ ĻĖ░ņ×¼ĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö ņĀĆņ×ÉĻ░Ć ņåīņåŹļÉ£ ĻĖ░Ļ┤ĆņØś ņŚ░ĻĄ¼ņ£żļ”¼ņŗ¼ņØśņ£äņøÉĒÜīņØś ņŖ╣ņØĖņØä ļ░øņĢśļŗż(ņŖ╣ņØĖļ▓łĒśĖ: EMCS 2023-01-021).
Ļ▓Ć ņé¼
ņĖĪļæÉĻ│© CTļŖö GE HealthCare (Chicago, IL, USA)ņØś SOMATOMņ£╝ļĪ£ 120 kV (ņĄ£ļīĆ), 86 mA, 0.6 mm ņŖ¼ļØ╝ņØ┤ņŖż ļæÉĻ╗śļĪ£ ņ┤¼ņśüĒĢśņśĆĻ│Ā ņśüņāüņØśĒĢÖĻ│╝ņØś ņĀĢņŗØ ĒīÉļÅģņØä ĻĘ╝Ļ▒░ļĪ£ CT ņåīĻ▓¼ņØä ļČäņäØĒĢśņśĆļŗż. ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ļŖö ĻĖ░ļÅäņÖĆ Ļ│©ļÅäņŚÉ ļīĆĒĢ┤ ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, 250, 500, 1000, 2000, 3000, 4000 Hzļź╝ ĻĖ░ļĪØĒĢśņśĆļŗż. ĻĖ░ļÅäĻ│©ļÅäņ░©ļŖö ļ»ĖĻĄŁ ņØ┤ļ╣äņØĖĒøäĻ│╝-ļæÉĻ▓ĮļČĆņÖĖĻ│╝ĒĢÖĒÜī(American Academy of Otolaryngology-Head and Neck Surgery)ņØś Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉ ļö░ļØ╝ 500, 1000, 2000, 3000 HzņŚÉņä£ ĻĖ░ļÅä ņ▓ŁļĀźĻ│╝ Ļ│©ļÅä ņ▓ŁļĀźņØś ĒÅēĻĘĀ ņ░©ņØ┤ļĪ£ Ļ│äņé░ĒĢśņśĆļŗż[15]. ļśÉĒĢ£, ņĄ£ņĀüņĢłņĀĢņŚŁņ╣śņŚÉņä£ ņĖĪņĀĢĒĢ£ ņ¢┤ņØīļ¬ģļŻīļÅäļź╝ ļČäņäØņŚÉ ĒżĒĢ©ņŗ£ņ╝░ļŗż. ĻĖ░ļÅäĻ│©ļÅä ņ░© ņśüņŚŁņØä ņŻ╝Ēīīņłśļ│äļĪ£ ļČäļźśĒĢśņśĆļŖöļŹ░, ņĀĆņØīņŚŁļīĆļŖö 250, 500, 1000 kHz ņżæ ņŚ░ņåŹļÉ£ ļæÉ ņŻ╝ĒīīņłśņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░©Ļ░Ć 20 dB ņØ┤ņāüņØ╝ ļĢī, Ļ│ĀņØīņŚŁļīĆļŖö 2000, 3000, 4000 Hz ņżæ ņŚ░ņåŹļÉ£ ļæÉ ņŻ╝ĒīīņłśņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░©Ļ░Ć 20 dB ņØ┤ņāüņØ╝ ļĢīļĪ£ ņĀĢņØśĒĢśņśĆļŗż[16]. Ļ│ĀņŗżļÅä Ļ▓Ćņé¼ļŖö -100~+100 mmH2OņŚÉņä£ ņĄ£ļīĆ Ēāäņä▒ņØ┤ Ļ┤Ćņ░░ļÉśļŖö Ļ▓āņØä AĒśĢ, ņĄ£ļīĆ Ēāäņä▒ņØ┤ AņÖĆ Ļ░ÖņØĆ ļ▓öņ£äņŚÉ ņ׳ņ£╝ļéś Ēāäņä▒ņØś ļ│ĆĒÖöĻ░Ć 0.3 mL ļ»Ėļ¦īņØĖ Ļ▓ĮņÜ░ As, ņĄ£ļīĆ Ēāäņä▒ņØ┤ AņÖĆ Ļ░ÖņØĆ ļ▓öņ£äņŚÉ ņ׳ņ£╝ļéś Ēāäņä▒ņØś ļ│ĆĒÖöĻ░Ć 1.5 mL ņ┤łĻ│╝ņØĖ Ļ▓ĮņÜ░ Ad, ņĄ£ļīĆ Ēāäņä▒ņØ┤ -100 mmH2O ļ»Ėļ¦īņŚÉņä£ Ļ┤Ćņ░░ļÉśļŖö Ļ▓āņØä CĒśĢņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż.
ĒåĄĻ│ä ļČäņäØ
ĒåĄĻ│ä ļČäņäØņØĆ SPSS ļ▓äņĀä 18.0 (SPSS I nc., C hicago, IL, USA)ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļČäņäØĒĢśņśĆļŗż. ņØĖĻĄ¼ĒĢÖņĀü ĒŖ╣ņä▒ Ļ░ä ļ╣łļÅä ņ░©ņØ┤ļź╝ ļČäņäØĒĢśĻĖ░ ņ£äĒĢ┤ Žć2-testņÖĆ ļĪ£ņ¦ĆņŖżĒŗ▒ ĒÜīĻĘĆļČäņäØņØä ņØ┤ņÜ®ĒĢśņśĆĻ│Ā, ņĖĪļæÉĻ│© CT ņåīĻ▓¼ņŚÉ ļö░ļźĖ ņ▓ŁļĀźļÅä ļ╣äĻĄÉļź╝ ņ£äĒĢ┤ independent t-testļź╝ ņØ┤ņÜ®ĒĢśņśĆĻ│Ā, ņłśņłĀ ņĀäĒøä ņ▓ŁļĀźņŚŁņ╣śņØś ļ╣äĻĄÉņÖĆ ņłśņłĀ Ēøä ĻĖ░ļÅäĻ│©ļÅäņ░©ņØś ļ│ĆĒÖöļź╝ ņŻ╝Ēīīņłśļ│äļĪ£ ļ╣äĻĄÉĒĢśĻĖ░ ņ£äĒĢ┤ paired t-testļź╝ ņØ┤ņÜ®Ē¢łļŗż. ņŻ╝Ēīīņłśļ│ä ļ╣äĻĄÉļŖö Bonferroni ĻĄÉņĀĢņØä ņĀüņÜ®ĒĢ£ p’╝£0.005ļź╝ ņ£ĀņØśņłśņżĆņ£╝ļĪ£ ĒĢśņśĆĻ│Ā ļéśļ©Ėņ¦Ć ĒåĄĻ│äļŖö p’╝£0.05ļź╝ ņ£ĀņØśņłśņżĆņ£╝ļĪ£ ĒĢśņśĆļŗż.
Ļ▓░ Ļ│╝
ņØĖĻĄ¼ĒĢÖņĀü ĒŖ╣ņä▒
66ļ¬ģ ĒÖśņ×ÉļōżņØś ļéśņØ┤ļŖö 18ņäĖņŚÉņä£ 72ņäĖĻ╣īņ¦Ć ļČäĒżĒĢśņśĆĻ│Ā, ĒÅēĻĘĀņØĆ 46.8┬▒17.0ņäĖņśĆļŗż(Table 1). ņØ┤ ņżæ 38ļ¬ģ(57.6%)ņØ┤ ņŚ¼ņ×ÉņśĆĻ│Ā, 28ļ¬ģ(42.4%)ņØ┤ ņÜ░ņĖĪ ĻĘĆņśĆļŗż. ņ¢æņĖĪļ│┤ļŗżļŖö ņØ╝ņĖĪ ņ▓ŁļĀźņĀĆĒĢśņØś ļ╣łļÅäĻ░Ć ļåÆņĢśĻ│Ā(Žć2 [2, 66]=8.27, p=0.02), ņóīņÜ░ Ļ░äņŚÉ ņ░©ņØ┤ļŖö ņŚåņŚłļŗż(p’╝×0.05). ĻĖ░ļÅäĻ│©ļÅäņ░©ļŖö ĒÅēĻĘĀ 24.8┬▒10.3 dBļĪ£ 10-19 dBņŚÉ 24ļ¬ģ(36.4%), 20-29 dBņŚÉ 22ļ¬ģ(33.3%), 30-39 dBņØĆ 11ļ¬ģ(16.7%), 40 dB ņØ┤ņāüņØĆ 9ļ¬ģ(13.6%) ļČäĒżĒĢśņśĆļŗż. ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ļ│┤ņØ┤Ļ│Ā ņŚ░ņåŹļÉ£ ļæÉ ņŻ╝ĒīīņłśņŚÉņä£ Ļ│©ļÅäņ▓ŁļĀźņØ┤ 25 dBņØä ņ┤łĻ│╝ĒĢśļŖö Ļ▓ĮņÜ░ Ēś╝ĒĢ®ņä▒ ļé£ņ▓Łņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆĻ│Ā, ņĀäņØīņä▒ ļé£ņ▓ŁĻ│╝ Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØś ļ╣äņ£©ņØĆ Ļ░üĻ░ü 28ļ¬ģ(42.4%), 38ļ¬ģ(57.6%)ļĪ£ ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłĻ│Ā(p’╝×0.05), ņŚ░ļĀ╣ņØ┤ ņ”ØĻ░ĆĒĢĀņłśļĪØ Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØä ļ│┤ņØ╝ ĒÖĢļźĀņØ┤ ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż(OR=1.07, 95% CI 1.028-1.106, p’╝£0.05). ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ņŻ╝Ēīīņłśļ│äļĪ£ ļéśļłäņŚłņØä ļĢī, ņĀĆņØīņŚŁļīĆļŖö 29ļ¬ģ(43.9%), ņĀäņØīņŚŁļīĆļŖö 37ļ¬ģ(56.1%), Ļ│ĀņØīņŚŁļīĆļŖö 0ĻĘĆņśĆļŗż(Table 1).
ņłśņłĀņØä ĒåĄĒĢ£ ņ¦äļŗ©Ļ│╝ ņĖĪļæÉĻ│© CT Ļ▓░Ļ│╝
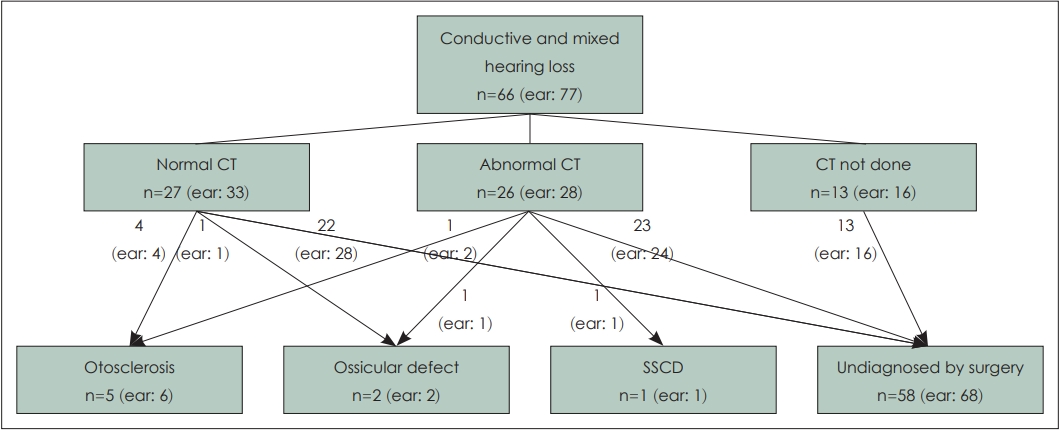
66ļ¬ģņØś ĒÖśņ×ÉņØś 77ĻĘĆ ņżæ ņłśņłĀļĪ£ ņ¦äļŗ©ļ¬ģņØ┤ ĒÖĢņØĖļÉ£ Ļ▓ĮņÜ░Ļ░Ć 10ĻĘĆ ņ׳ņŚłĻ│Ā, ņØ┤Ļ▓ĮĒÖöņ”Ø 6ĻĘĆ, ņØ┤ņåīĻ│©ņŚ░ņćä ļŗ©ņĀł 2ĻĘĆ, ņāüļ░śĻ│Āļ”¼ Ļ┤ĆĒö╝ņŚ┤ņ”ØĒøäĻĄ░ 1ĻĘĆ, ņøÉņØĖļ»Ėņāü 1ĻĘĆņśĆļŗż(Fig. 1 and Table 1). ņ┤Ø 77ĻĘĆ(66ļ¬ģ) ņżæ ņĖĪļæÉĻ│© CTļź╝ ņ┤¼ņśüĒĢ£ 61ĻĘĆ(53ļ¬ģ)ļź╝ ļīĆņāüņ£╝ļĪ£ CT ņåīĻ▓¼ņØä ļČäņäØĒĢ£ Ļ▓░Ļ│╝ ņĀĢņāü ņåīĻ▓¼ņØ┤ 33ĻĘĆ(54.1%), ļ╣äņĀĢņāü ņåīĻ▓¼ņØ┤ 28ĻĘĆ(45.9%)ņśĆļŗż(Table 2). ņĀĢņāü ņåīĻ▓¼ĻĄ░Ļ│╝ ļ╣äņĀĢņāü ņåīĻ▓¼ĻĄ░ Ļ░äņŚÉ ņä▒ļ│ä, ļéśņØ┤, ļ░®Ē¢źņä▒, ņĀäņØīņä▒Ļ│╝ Ēś╝ĒĢ®ņä▒ ļé£ņ▓Ł ļ╣äņ£©ņØĆ ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤ļŖö ņŚåņŚłļŗż(p’╝×0.05). ņĖĪļæÉĻ│© CT ņĀĢņāü ņåīĻ▓¼ĻĄ░ 33ĻĘĆ ņżæ ņłśņłĀļĪ£ ņ¦äļŗ©ņØ┤ ĒÖĢņØĖļÉ£ Ļ▓ĮņÜ░ļŖö ņØ┤Ļ▓ĮĒÖöņ”Ø 4ĻĘĆ(12.1%), ņØ┤ņåīĻ│© ņŚ░ņćäļŗ©ņĀł 1ĻĘĆ(3.0%)Ļ░Ć ņ׳ņŚłĻ│Ā, ļéśļ©Ėņ¦Ć 28ĻĘĆ(84.8%)ņØĆ ņ¦äļŗ©ņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 1). ņĖĪļæÉĻ│© CTņŚÉņä£ ļéśĒāĆļé£ ļ╣äņĀĢņāü ņåīĻ▓¼ņØĆ Table 2ņÖĆ Ļ░Öļŗż. ņĖĪļæÉĻ│© CT ļ╣äņĀĢņāü ņåīĻ▓¼ ĒÖśņ×É 28ĻĘĆ ņżæ ņłśņłĀņØä ĒåĄĒĢ┤ ņ¦äļŗ©ļÉ£ Ļ▓ĮņÜ░ļŖö ņØ┤Ļ▓ĮĒÖöņ”Ø 2ĻĘĆ(7.1%), ņØ┤ņåīĻ│© ĻĖ░ĒśĢ 1ĻĘĆ(3.6%), ņāüļ░śĻ│Āļ”¼Ļ┤ĆĒö╝ņŚ┤ņ”ØĒøäĻĄ░ 1ĻĘĆ(3.6%)Ļ░Ć ņ׳ņŚłĻ│Ā ļéśļ©Ėņ¦Ć 24ĻĘĆ(85.7%)ļŖö ņ¦äļŗ©ņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 1). ņłśņłĀņØä ĒåĄĒĢ┤ ņØ┤Ļ▓ĮĒÖöņ”Øņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ 6ĻĘĆ ņżæ ņĖĪļæÉĻ│© CTņŚÉņä£ ņØ┤ņāü ņåīĻ▓¼ņØ┤ ļ│┤ņØĖ Ļ▓āņØĆ 2ĻĘĆ ņ׳ņŚłļŗż.
ņ×äņāüņĀü ņ¦äļŗ©
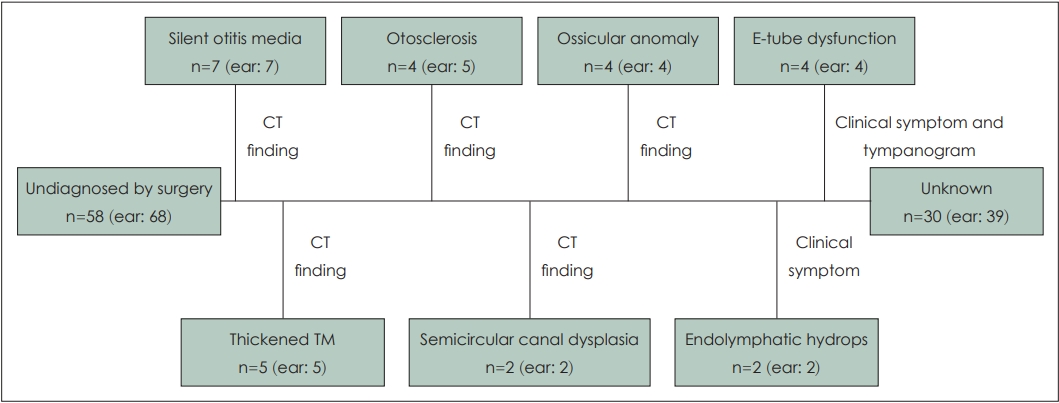
ņłśņłĀļĪ£ ņ¦äļŗ©ņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņØĆ ņśłļōżņØĆ ņĖĪļæÉĻ│© CT, Ļ│ĀņŗżļÅä Ļ▓Ćņé¼, ņ▓ŁļĀźļÅäņØś ņ¢æņāü, ļÅÖļ░ś ņ”ØņāüņØä ĒåĀļīĆļĪ£ ņ¦äļŗ©ņØ┤ ņČöņĀĢ Ļ░ĆļŖźĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö ņ×äņāüņĀü ņ¦äļŗ©ļ¬ģņØä ļČÖņØ┤Ļ│Ā ĻĘĖ ļéśļ©Ėņ¦Ćļź╝ ļ»Ėņāü(unknown) ņ£╝ļĪ£ ņ¦æĻ│äĒĢśņśĆļŗż. ņĖĪļæÉĻ│© CTņŚÉņä£ ņØ┤Ļ▓ĮĒÖöņ”ØņØä ņŗ£ņé¼ĒĢśĻ▒░ļéś, ņØ┤ņåīĻ│© ĻĖ░ĒśĢ, ļé┤ņØ┤ ĻĖ░ĒśĢ, Ļ│Āļ¦ē ļ╣äĒøä, Ļ▓ĮĒÖöņä▒ ņ£Āņ¢æļÅÖ ļō▒ņØś ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ĻĘĖ ņåīĻ▓¼ņŚÉ ļö░ļØ╝ ņ×äņāüņĀü ņ¦äļŗ©ļ¬ģņØä ļČÖņśĆļŗż. ņØ┤ņČ®ļ¦īĻ░É ļśÉļŖö ņ╣©ņØä ņé╝ĒéżļŖö ļÅÖņ×æņŚÉņä£ Ēä░ņ¦ĆļŖö ņåīļ”¼ņÖĆ ĒĢ©Ļ╗ś Ļ│ĀņŗżļÅä Ļ▓Ćņé¼ņŚÉņä£ CĒśĢņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ņØ┤Ļ┤ĆĻĖ░ļŖźņןņĢĀļĪ£ ņ¦äļŗ©ĒĢśņśĆļŗż[17]. ņĀĆņØīņŚŁļīĆ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ļ│┤ņØ┤ļŖö ĒÖśņ×É ņżæ ņØ┤ņČ®ļ¦īĻ░É, ņØ┤ļ¬ģ, ņ¢┤ņ¦Ćļ¤╝ņ”Ø ņżæ ļæÉ Ļ░Ćņ¦Ć ņØ┤ņāüņØś ņ”ØņāüņØä ļéśĒāĆļéĀ ļĢī ļé┤ļ”╝Ēöäņłśņóģņ£╝ļĪ£ ņ¦äļŗ©ĒĢśņśĆļŗż[16,18]. ņØ┤ļ¤¼ĒĢ£ Ļ│╝ņĀĢņØä ĒåĄĒĢ┤ ņłśņłĀņĀüņ£╝ļĪ£ ņ¦äļŗ©ļ¬ģņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŹś 68ĻĘĆ ņżæ ņ×Āļ│Ąņä▒ ņżæņØ┤ņŚ╝ 7ĻĘĆ(10.3%), Ļ│Āļ¦ē ļ╣äĒøä 5ĻĘĆ(7.4%), ņØ┤Ļ▓ĮĒÖöņ”Ø 5ĻĘĆ(7.4%), ņØ┤ņåīĻ│© ĻĖ░ĒśĢ 4ĻĘĆ(5.9%), ņØ┤Ļ┤ĆĻĖ░ļŖźņןņĢĀ 4ĻĘĆ(5.9%), ļ░śĻ│Āļ”¼Ļ┤Ć ĻĖ░ĒśĢ 2ĻĘĆ(2.9%), ļé┤ļ”╝Ēöäņłśņóģ 2ĻĘĆ(2.9%)ļĪ£ ņ┤Ø 29ĻĘĆ(42.6%)Ļ░Ć ņ×äņāüņĀüņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 2 and Table 3).
ņ▓ŁļĀź Ļ▓░Ļ│╝
ņĖĪļæÉĻ│© CT ņåīĻ▓¼ņŚÉ ļö░ļØ╝ ņĀĢņāüņåīĻ▓¼ĻĄ░Ļ│╝ ļ╣äņĀĢņāüņåīĻ▓¼ĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼ļź╝ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī ĻĖ░ļÅä ņ▓ŁļĀź, Ļ│©ļÅä ņ▓ŁļĀź, ĻĖ░ļÅäĻ│©ļÅäņ░©ņŚÉņä£ ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļŖö ņŚåņŚłņ£╝ļéś(p’╝×0.05), ņ¢┤ņØīļ¬ģļŻīļÅäļŖö ļ╣äņĀĢņāü ņåīĻ▓¼ĻĄ░ņØ┤ ņĀĢņāü ņåīĻ▓¼ĻĄ░ļ│┤ļŗż ņ£ĀņØśļ»ĖĒĢśĻ▓ī ņĀĆĒĢśļÉśņ¢┤ ņ׳ņŚłļŗż(86.5%┬▒10.7% vs. 92.8┬▒13.1; t[58]=1.8, p’╝£0.05) (Table 4). ņĀäņØīņä▒ ļé£ņ▓ŁĻ│╝ Ēś╝ĒĢ®ņä▒ ļé£ņ▓Łņé¼ņØ┤ņŚÉ ĻĖ░ļÅäĻ│©ļÅäņ░©ņÖĆ ņ¢┤ņØīļ¬ģļŻīļÅäņØś ņ░©ņØ┤ļŖö ņŚåņŚłņ£╝ļ®░(p’╝×0.05), ņØ╝ņĖĪņä▒ ļé£ņ▓ŁĻ│╝ ņ¢æņĖĪņä▒ ļé£ņ▓Ł ņé¼ņØ┤ņŚÉņä£ļŖö ĻĖ░ļÅä ņ▓ŁļĀź, Ļ│©ļÅä ņ▓ŁļĀź, ĻĖ░ļÅäĻ│©ļÅäņ░©ņÖĆ ņ¢┤ņØīļ¬ģļŻīļÅäņØś ņ░©ņØ┤ļŖö ņŚåņŚłļŗż(p’╝×0.05).
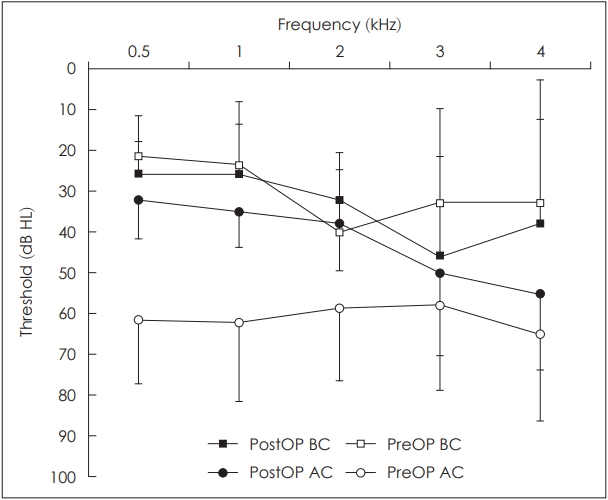
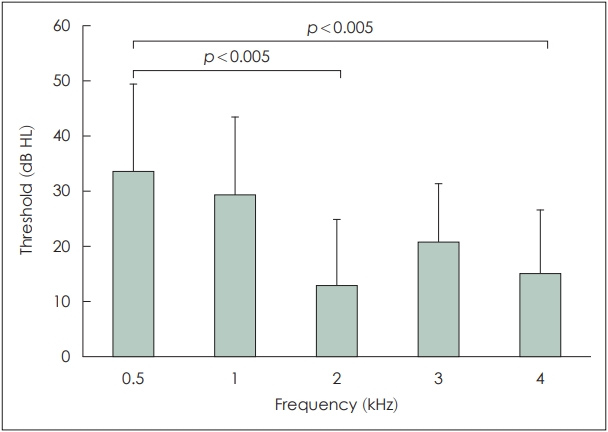
ņłśņłĀ ņĀäĒøä Ļ│©ļÅä ņ▓ŁļĀźņØĆ Ļ░üĻ░ü 29.5┬▒15.2 dBņÖĆ 32.3┬▒12.1 dBļĪ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ¦Ćļ¦ī(p’╝×0.05), ĻĖ░ļÅä ņ▓ŁļĀźņØĆ ņłśņłĀ ņĀä 60.0┬▒17.7 dB HLņŚÉņä£ ņłśņłĀ Ēøä 38.8┬▒10.0 dBļĪ£ ņ£ĀņØśļ»ĖĒĢ£ Ļ░Éņåīļź╝ ļ│┤ņśĆĻ│Ā(t[6]=3.29, p=0.01), ĻĖ░ļÅäĻ│©ļÅäņ░©ļÅä ņłśņłĀ ņĀä 30.5┬▒12.7 dBņŚÉņä£ 6.4┬▒4.0 dBļĪ£ ņ£ĀņØśļ»ĖĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(t[6]=6.29, p’╝£0.05) (Fig. 3 and Table 5). Subject 3ņØś Ļ▓ĮņÜ░ ņŗ£ĒŚśņĀü Ļ│ĀņŗżĻ░£ļ░®ņłĀļĪ£ ņØ┤Ļ▓ĮĒÖöņ”Øņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłĻ│Ā ņØ┤ņ░© ņłśņłĀņØä Ļ│äĒÜŹĒĢśņśĆņ£╝ļéś ņČöņĀü ĒāłļØĮļÉśņŚłļŗż. Ļ│ĀņŗżĻ░£ļ░®ņłĀļĪ£ ļ│æļ│ĆņØä ļ░£Ļ▓¼ĒĢśņ¦Ć ļ¬╗ĒĢ£ subject 9Ļ│╝ ņłśņłĀ Ēøä ņ▓ŁļĀźļÅäĻ░Ć ņŚåļŖö subject 3Ļ│╝ 4ļź╝ ņĀ£ņÖĖĒĢśĻ│Ā Ļ░ü ņŻ╝Ēīīņłśļ│äļĪ£ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī, ņłśņłĀ ĒøäņŚÉ ļ¬©ļōĀ ņŻ╝ĒīīņłśņŚÉņä£ ņ£ĀņØśļ»ĖĒĢ£ ĻĖ░ļÅäĻ│©ļÅäņ░© Ļ░Éņåīļź╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż(p’╝£0.05). ņłśņłĀ Ēøä ņŻ╝Ēīīņłśļ│ä ĻĖ░ļÅäĻ│©ļÅäņ░©ņØś Ļ░ÉņåīĒÅŁņØĆ 0.5 kHzņÖĆ 2 kHz, ĻĘĖļ”¼Ļ│Ā 0.5 kHzņÖĆ 4 kHz ņé¼ņØ┤ņŚÉņä£ Bonferroni ņłśņĀĢ ņ£ĀņØśņłśņżĆņØä ļ¦īņĪ▒ĒĢśļŖö ņ░©ņØ┤ļź╝ ļ│┤ņśĆļŗż(’╝£0.005, accepted p value=0.05/10=0.005) (Fig. 4). 0.5 kHzņÖĆ 1 kHzņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░© Ļ░ÉņåīĒÅŁņØś ĒĢ®Ļ│╝ 3 kHzņÖĆ 4 kHzņŚÉņä£ ĻĖ░ļÅäĻ│©ļÅäņ░© Ļ░ÉņåīĒÅŁņØś ĒĢ®ņØä ļ╣äĻĄÉĒĢ┤ ļ│┤ļ®┤ ļé«ņØĆ ļæÉ ņŻ╝ĒīīņłśņŚÉņä£ņØś Ļ░ÉņåīĒÅŁņØ┤ ņØśļ»Ė ņ׳Ļ▓ī Ēü░ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż(p=0.001).
Ļ│Ā ņ░░
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļ╣äņÖĖņāüņä▒ ļé£ņ▓ŁļōżņØś ĒÅēĻĘĀļéśņØ┤ļŖö 46.8ņäĖļĪ£ ļ╣äņŖĘĒĢ£ ļīĆņāüņ£╝ļĪ£ ņ¦äĒ¢ēĒĢ£ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ņŚÉņä£ ļéśĒāĆļé£ 25-41ņäĖņŚÉ ļ╣äĒĢśņŚ¼ ļåÆņØĆ ĒÄĖņØĖļŹ░ ņØ┤Ļ▓āņØĆ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØ┤ ņĀ£ņÖĖļÉśņŚłĻ▒░ļéś[10,19] ņÖĖņāüņä▒ ļé£ņ▓ŁņØ┤ ĒżĒĢ©ļÉśņŚłĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ļ│┤ņØĖļŗż[12,14,20,21]. ļśÉĒĢ£ ļ│Ė ņŚ░ĻĄ¼ ļīĆņāüņØĆ ņłśņłĀĒĢśņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉļōżļÅä ĒżĒĢ©ĒĢśņśĆĻ│Ā Ļ│ĀļĀ╣ņĖĄņŚÉņä£ ņłśņłĀņØä ļ░øņ¦Ć ņĢŖļŖö Ļ▓ĮĒ¢źņØ┤ ĒÅēĻĘĀļéśņØ┤ļź╝ ļåÆņØĖ ņøÉņØĖņØ┤ ļÉĀ ņłś ņ׳ļŗż.
ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļé£ņ▓ŁņØś ņøÉņØĖņ£╝ļĪ£ļŖö ņÖĖņØ┤ļÅä ļ│æļ│ĆņØä ņĀ£ņÖĖĒĢśļ®┤ ņØ┤Ļ▓ĮĒÖöņ”Ø, ņäĀņ▓£ņä▒ ņØ┤ņåīĻ│© Ļ│ĀņĀĢ, ņØ┤ņåīĻ│© ĻĖ░ĒśĢ, ņÖĖņāüņä▒ ņØ┤ņåīĻ│© ņåÉņāü ļō▒ ņżæņØ┤Ļ░Ģ ļé┤ ļ│æļ│ĆņØ┤ ĒØöĒĢśņ¦Ćļ¦ī[10,12] ļō£ļ¼╝Ļ▓ī ņāüļ░śĻ│Āļ”¼Ļ┤ĆĒö╝ņŚ┤ņ”ØĒøäĻĄ░, ņĀäņĀĢņłśļÅäĻ┤ĆĒÖĢņןņ”ØĒøäĻĄ░, Gusher ņ”ØĒøäĻĄ░, Paget ļ│æ, ļé┤ņØ┤ ļśÉļŖö ņ£Āņ¢æļÅīĻĖ░ņØś ļ│æļ│ĆļÅä ņ׳ļŗż[22]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņłśņłĀļĪ£ ĒÖĢņ¦äļÉ£ ņśł ņżæņŚÉļŖö ņØ┤Ļ▓ĮĒÖöņ”ØņØ┤ Ļ░Ćņן ĒØöĒ¢łļŗż. ņØ┤ņĀä ņŚ░ĻĄ¼ļōżņŚÉņä£ļÅä ņĀĢņāü Ļ│Āļ¦ēņØä Ļ░Ćņ¦ä ņĀäņØīņä▒ ļé£ņ▓Ł ĒÖśņ×ÉļōżņØä ņłśņłĀĒ¢łņØä ļĢī ņØ┤Ļ▓ĮĒÖöņ”ØņØ┤ Ļ░Ćņן ĒØöĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆĻ│Ā(27%-66%), ļō▒Ļ│© ņØ┤ņÖĖņØś ņØ┤ņåīĻ│© Ļ│ĀņĀĢ, ņØ┤ņåīĻ│©ņŚ░ņćä ļŗ©ņĀł ļśÉļŖö ĒāłĻĄ¼Ļ░Ć ļŗżņØīņ£╝ļĪ£ ĒØöĒĢ£ ņøÉņØĖņØä ņ░©ņ¦ĆĒĢśņśĆĻ│Ā(10%-30%), ņ¦äņŻ╝ņóģ, Ļ│Āņŗżņé¼ĻĄ¼ņóģ ļō▒ ņśłņāüĒĢśņ¦Ć ļ¬╗ĒĢ£ ņżæņØ┤ ļ│æļ│ĆņØ┤ ļ░£Ļ▓¼ļÉśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ņŚłļŗż[13,19,21]. ņÖĖņāü ņØ┤Ēøä ļ░£ņāØĒĢ£ ņĀäņØīņä▒ ļé£ņ▓Ł ĒÖśņ×ÉņŚÉņä£ļŖö ņØ┤ņåīĻ│© ĒāłĻĄ¼Ļ░Ć ĒØöĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[12,14]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņĪ░Ļ▒┤ņØä ļ¦īņĪ▒ĒĢśļŖö ņ”ØļĪĆļōżņØĆ ņ¢æņĖĪņä▒(10ļ¬ģ, 15.2%)ņŚÉ ļ╣äĒĢśņŚ¼ ņØ╝ņĖĪņä▒(56ļ¬ģ, 84.8%)ņØ┤ Ēø©ņö¼ ļåÆņØĆ ļ╣äņ£©ņØä ļ│┤ņśĆĻ│Ā ļŗżļźĖ ņŚ░ĻĄ¼ļōżņŚÉņä£ļÅä ņØ╝ņĖĪņä▒ņØś ļ╣äņ£©ņØ┤ ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[12,14,20]. ņØ┤Ļ▓ĮĒÖöņ”ØņØĆ ņ¢æņĖĪņä▒ņØ┤ ļŹö ĒØöĒĢ£ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ¦Ćļ¦ī[11] ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņØ┤Ļ▓ĮĒÖöņ”ØņØĆ ņłśņłĀļĪ£ ĒÖĢņØĖļÉ£ 6ĻĘĆņŚÉ CTļĪ£ļ¦ī ņØśņŗ¼ļÉ£ 5ĻĘĆļź╝ ĒżĒĢ©ĒĢśņŚ¼ļÅä ņ┤Ø 11ĻĘĆļĪ£ ĻĘĖ ļ╣äņ£©ņØ┤ ļåÆņ¦Ć ņĢŖņ£╝ļ»ĆļĪ£ ņĀäņ▓┤ņĀüņ£╝ļĪ£ ņ¢æņĖĪņä▒ņØś ļ╣äņ£©ņØ┤ ņĀüĻ▓ī ļéśĒāĆļé£ ņøÉņØĖņØś ĒĢśļéśļØ╝Ļ│Ā ņāØĻ░üļÉ£ļŗż. ļō▒Ļ│©Ļ│ĀņĀĢ ņåīĻ▓¼ņØĆ ņØ┤Ļ▓ĮĒÖöņ”Ø ņØ┤ņÖĖņŚÉļÅä ņäĀņ▓£ņä▒ ļō▒Ļ│©Ļ│ĀņĀĢņØś Ļ░ĆļŖźņä▒ļÅä ņ׳Ļ│Ā Pagetļ│æņŚÉņä£ ļÅÖļ░śļÉĀ ņłśļÅä ņ׳ņ¦Ćļ¦ī[23] ņ×äņāüņĀüņ£╝ļĪ£ ņ▓ŁļĀźņĀĆĒĢśĻ░Ć 20ļīĆļČĆĒä░ ņ¦äĒ¢ēņä▒ņ£╝ļĪ£ ļ░£ņāØĒĢśĻ│Ā ņ▓ŁļĀźĻ▓Ćņé¼ņŚÉņä£ Carhart ņĀł(notch)ņØ┤ ļ│┤ņØ┤Ļ▒░ļéś ņĖĪļæÉĻ│© CTņŚÉņä£ ņĀäņ░ĮņåīņŚ┤ņØ┤ļéś ņÖĆņÜ░ ņŻ╝ļ│Ć ņĀĆņØīņśü ļō▒ ĒŖ╣ņĀĢ ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ņĪ░ņ¦üĒĢÖņĀü ņ¦äļŗ©ņØ┤ ņŚåļŹöļØ╝ļÅä ņØ┤Ļ▓ĮĒÖöņ”ØņØä Ļ░ĢĒĢśĻ▓ī ņØśņŗ¼ĒĢĀ ņłś ņ׳ļŗż[11,24,25]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņłśņłĀ ņåīĻ▓¼ņŚÉņä£ ļō▒Ļ│© Ļ│ĀņĀĢņØ┤ ĒÖĢņØĖļÉ£ ĒÖśņ×ÉļōżņØĆ ļ¬©ļæÉ ņØ┤Ļ▓ĮĒÖöņ”ØņØś ņ×äņāüņ¢æņāüņŚÉ ļČĆĒĢ®ĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤Ļ▓ĮĒÖöņ”Øņ£╝ļĪ£ ļČäļźśĒĢśņśĆļŗż. ļśÉĒĢ£ ņłśņłĀļĪ£ ņ¦äļŗ©ļÉ£ ņØ┤Ļ▓ĮĒÖöņ”Ø 6ĻĘĆ(5ļ¬ģ) ņżæ ņłśņłĀ ņĀäņŚÉ ņĖĪļæÉĻ│© CTļź╝ ĒåĄĒĢ┤ ņØ┤Ļ▓ĮĒÖöņ”ØņØä ņØśņŗ¼ĒĢĀ ņłś ņ׳ņŚłļŹś Ļ▓ĮņÜ░ļŖö ĒĢ£ ļ¬ģņØś 2ĻĘĆņŚÉ ļČłĻ│╝ĒĢśņśĆļŗż. ņØ┤ļŖö ĻĖ░ņĪ┤ ļ¼ĖĒŚīņŚÉņä£ ļ│┤ņØ┤ļŖö ņĖĪļæÉĻ│© CTņØś ļ»╝Ļ░ÉļÅä 60%-91%ņŚÉ[24,26] ļ╣äĒĢśņŚ¼ ņāüļŗ╣Ē׳ ļé«ņØĆ ĒÄĖņØĖļŹ░ ņØ┤Ļ▓āņØĆ ņØ┤Ļ▓ĮĒÖöņ”Øņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ ņłśĻ░Ć ņĀüņŚłĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ĒĢ£ ņśłņØś ņāüļ░śĻ│Āļ”¼Ļ┤ĆĒö╝ņŚ┤ņ”ØĒøäĻĄ░ņØ┤ ņłśņłĀņØä ĒåĄĒĢ┤ ĒÖĢņ¦äļÉśņŚłļŖöļŹ░ ņłĀņĀä ņ▓ŁļĀźĻ▓Ćņé¼ņŚÉņä£ 2 8.3 dBņØś ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆĻ│Ā 4 kHz ņØ┤ņāüņØś Ļ│ĀņŻ╝ĒīīņłśņŚÉņä£ļ¦ī Ļ│©ņĀäļÅäņŚŁņ╣śĻ░Ć ņāüņŖ╣ĒĢśļŖö Ēś╝ĒĢ®ņä▒ļé£ņ▓Ł ņ¢æņāüņØä ļ│┤ņśĆļŗż. ņāüļ░śĻ│Āļ”¼Ļ┤ĆĒö╝ņŚ┤ņ”ØĒøäĻĄ░ņØĆ ņĀäņĀĢņłśļÅäĻ┤ĆĒÖĢņןņ”ØĒøäĻĄ░Ļ│╝ ĒĢ©Ļ╗ś ņĀ£3ņØś ņ░Į(third window effect)ĒÜ©Ļ│╝ņŚÉ ņØśĒĢ£ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ļ│┤ņØ┤ļŖö ļé┤ņØ┤ņ¦łĒÖśņ£╝ļĪ£ Ēü░ņåīļ”¼ņÖĆ ņĢĢļĀźņŚÉ ņ£Āļ░£ļÉśļŖö ņ¢┤ņ¦Ćļ¤¼ņøĆņ”Ø, ņ▓ŁĻ░üĻ│╝ļ»╝ ļō▒ņØś ļÅÖļ░śņ”ØņāüņØä ĒåĄĒĢ£ ņØśņŗ¼Ļ│╝ ņāüļ░śĻ│Āļ”¼Ļ┤ĆņØś ņןņČĢĻ│╝ ĒÅēĒ¢ēĒĢ£ Ļ┤Ćņāüļ®┤ CT ņ×¼ĻĄ¼ņä▒ ņØ┤ļ»Ėņ¦Ćļź╝ ĒåĄĒĢśņŚ¼ ņ¦äļŗ©ĒĢĀ ņłś ņ׳ļŗż[27,28]. ņŗ£ĒŚśņĀü Ļ│ĀņŗżĻ░£ļ░®ņłĀņŚÉņä£ ņøÉņØĖņØä ļ░£Ļ▓¼ĒĢĀ ņłś ņŚåļŖö ņśłĻ░Ć 10ĻĘĆ ņżæ 1ĻĘĆ ņ׳ņŚłļŖöļŹ░ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļÅä 3%-4%ļŖö ļ░£Ļ▓¼ļÉśņ¦Ć ļ¬╗ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[19,20].
ņĀĢņāüĻ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ĒÖśņ×ÉņŚÉņä£ ņłśņłĀļĪ£ ņ¦äļŗ©ņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░ ņĖĪļæÉĻ│© CTņÖĆ ļÅÖļ░śņ”ØņāüņØä ņ×ÉņäĖĒ׳ ļČäņäØĒĢ┤ ļ│┤ļ®┤ ņ×äņāüņĀü ņ¦äļŗ©ļ¬ģņØä ļČÖņØ╝ ņłś ņ׳ļŖö Ļ▓ĮņÜ░Ļ░Ć ņāüļŗ╣ņłś ņ׳ņŚłļŗż. ņĖĪļæÉĻ│© CTņŚÉņä£ Ļ▓ĮĒÖöņä▒ ņ£Āņ¢æļÅÖņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ņ×Āļ│Ąņä▒ ņżæņØ┤ņŚ╝ņ£╝ļĪ£ ņ¦äļŗ©ĒĢśņśĆĻ│Ā, ņØ┤ļ¤¼ĒĢ£ Ļ▓ĮņÜ░ ņżæņØ┤Ļ░Ģ ļé┤ņŚÉ ņ£ĪņĢłņ£╝ļĪ£ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņØĆ ņŚ╝ņ”ØņØ┤ ņ׳Ļ▒░ļéś Ļ│╝Ļ▒░ņØś ņŚ╝ņ”ØņØ┤ ĻĖ░ļÅäĻ│©ļÅäņ░©ņØś ņøÉņØĖņØ┤ ļÉĀ ņłś ņ׳ļŗż[29]. ļśÉ, Ļ│Āļ¦ēņØś ļ¬©ņ¢æņŚÉ ļ│ĆĒÖöļź╝ ņ┤łļלĒĢśņ¦Ć ņĢŖļŖö ņłśņżĆņØś ņØ┤Ļ┤ĆĻĖ░ļŖźņןņĢĀļØ╝ļÅä ņżæņØ┤ ļé┤ ņĢĢļĀźĻ░ÉņåīļĪ£ Ļ│Āļ¦ēĻ│╝ ņØ┤ņåīĻ│©ņØś ņÜ┤ļÅÖņä▒ņØ┤ Ļ░Éņåīņŗ£ņ╝£ ņĀäņØīņä▒ ļé£ņ▓ŁņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŗż[17]. ļé┤ļ”╝ĒöäņłśņóģņØś Ļ▓ĮņÜ░ņŚÉļÅä ņ”ØĻ░ĆĒĢ£ ļé┤ļ”╝Ēöä ņĢĢļĀźņØ┤ ļō▒Ļ│© ņøĆņ¦üņ×äņØś ņĀĆĒĢśņŗ£ņ╝£ ņĀĆņŻ╝Ēīīņłś ņśüņŚŁņŚÉ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ ņ£Āļ░£ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[16,18].
ņĖĪļæÉĻ│© CTņŚÉņä£ ļ╣äņĀĢņāü ņåīĻ▓¼ĻĄ░Ļ│╝ ņĀĢņāü ņåīĻ▓¼ĻĄ░Ļ│╝ ņ▓ŁļĀźņØä ļ╣äĻĄÉĒĢśņśĆņØä ļĢī Ļ│©ņĀäļÅä ņŚŁņ╣śņŚÉ ņ░©ņØ┤Ļ░Ć ņŚåņŚłĻ│Ā Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØś ļ╣äņ£©ļÅä ņ░©ņØ┤Ļ░Ć ņŚåņŚłņ£╝ļéś ņ¢┤ņØīļČäļ│äļĀźņØĆ ļ╣äņĀĢņāü ņåīĻ▓¼ĻĄ░ņŚÉņä£ ņ£ĀņØśļ»ĖĒĢśĻ▓ī ļé«ņĢśļŗż. ņĖĪļæÉĻ│© CTņØś ļ╣äņĀĢņāü ņåīĻ▓¼ļōż ņżæ ņ£Āņ¢æļÅÖ Ļ▓ĮĒÖöņ”ØņØ┤ļéś ļ╣äĒøäļÉ£ Ļ│Āļ¦ē ļō▒ ņ×Āļ│Ąņä▒ ņżæņØ┤ņŚ╝ņØ┤ļéś Ļ│╝Ļ▒░ņØś ņŚ╝ņ”ØņØä ņØśņŗ¼ĒĢĀ ņłś ņ׳ļŖö ņåīĻ▓¼ļōżņØ┤ ņ׳ņŚłļŖöļŹ░, ņØ┤ļ¤¼ĒĢ£ Ļ▓ĮņÜ░ Ļ│Āļ¦ēņŚÉ ņ£ĪņĢłņĀü ņØ┤ņāüņØä ņ┤łļלĒĢśņ¦Ć ņĢŖņĢśņØīņŚÉļÅä ņŚ╝ņ”ØņØ┤ ņןĻĖ░ņĀüņ£╝ļĪ£ ņ¢┤ņØīļČäļ│äļĀźņØä ļ¢©ņ¢┤ļ£©ļĀĖņØä Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż. ņĄ£ĻĘ╝ ņØ╝ņĖĪņŚÉļ¦ī ņĀäņØīņä▒ ļé£ņ▓ŁņØä Ļ░Ćņ¦ĆļŖö ņĮöĒśĖĒŖĖ ņŚ░ĻĄ¼ņŚÉņä£ ņĀäņØīņä▒ ļé£ņ▓ŁņĖĪ ĻĘĆĻ░Ć ņżæņØ┤Ļ░ĢņØ┤ļéś ņ£Āņ¢æļÅÖņŚÉ ļ¦īņä▒ņĀüņØĖ ņŚ╝ņ”ØņØä ļÅÖļ░śĒĢśļŖö Ļ▓ĮņÜ░, Ļ│©ņĀäļÅä ņŚŁņ╣śĻ░Ć ņĀĢņāüņØ┤ļŹöļØ╝ļÅä Ļ▒┤ņĖĪ ĻĘĆņŚÉ ļ╣äĒĢśņŚ¼ ņ¢┤ņØīļČäļ│äļĀźņØ┤ ņ£ĀņØśļ»ĖĒĢśĻ▓ī ņĀĆĒĢśļÉśņŚłļŖöļŹ░, ļ¦īņä▒ņĀü ņŚ╝ņ”ØņØ┤ Ļ│©ņĀäļÅäņŚŁņ╣śņŚÉ ņśüĒ¢źņØä ņŻ╝ņ¦Ć ņĢŖļŖö ņĀĢļÅäļØ╝ļÅä ļé┤ņØ┤ņåÉņāüņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ĻĘĖ ņøÉņØĖņØä ņČöņĀĢĒĢśņśĆļŗż[29]. ņłśņłĀ Ēøä ĻĖ░ļÅäņ▓ŁļĀźņØś Ļ░£ņäĀņØĆ ņĀĆņŻ╝Ēīī ļīĆņŚŁ(0.5 kHņÖĆ 1 kHz)ņŚÉņä£ Ļ│ĀņŻ╝Ēīī ļīĆņŚŁ(3 kHzņÖĆ 4 kHz)ļ│┤ļŗż Ēü░ Ļ▓ĮĒ¢źņØä ļ│┤ņśĆņ£╝ļéś ņ”ØļĪĆņłśĻ░Ć ņČ®ļČäĒĢśņ¦Ć ņĢŖņĢä Ļ▓░ļĪĀ ļé┤ļ”¼ĻĖ░ļŖö ņ¢┤ļĀĄļŗż. ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ņŚÉņä£ ņłśņłĀ Ēøä ĻĖ░ļÅäņ▓ŁļĀź Ļ░£ņäĀņØ┤ Ļ│ĀĒīīņłś ļīĆņŚŁņŚÉņä£ ņāüļīĆņĀüņ£╝ļĪ£ ņĀüņØĆ Ļ▓āņØä ļ│┤Ļ│ĀĒĢśņśĆļŖöļŹ░[30], ņłśņłĀ ņżæ ļō£ļ”┤ļ¦ü, ņØ┤ņåīĻ│© ņĪ░ņ×æ, ļĀłņØ┤ņĀĆņØś ņé¼ņÜ® ļō▒ņØ┤ Ļ│ĀņŻ╝Ēīī ļīĆņŚŁņŚÉ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ ļé£ņ▓ŁņØä ņ£Āļ░£ĒĢśņśĆņØä Ļ░ĆļŖźņä▒ņØä ņĀ£ņŗ£ĒĢśņśĆļŗż.
ļ│Ė ņŚ░ĻĄ¼ņØś ĒĢ£Ļ│äņĀÉņØĆ ņŚ░ĻĄ¼Ļ░Ć ĒøäĒ¢źņĀüņ£╝ļĪ£ ņ¦äĒ¢ēļÉśņŚłņ£╝ļ®░, ņłśņłĀņØä ļ░øņØĆ Ēæ£ļ│ĖņłśĻ░Ć ņĀüņ¢┤ņä£ ņĄ£ņóģņĀüņØĖ ņ¦äļŗ©ļ¬ģņØä ņĢī ņłś ņŚåļŖö ņśłĻ░Ć ļ¦ÄņĢśļŗżļŖö ņĀÉņØ┤ļŗż. ĒĢśņ¦Ćļ¦ī ņłśņłĀ ņŚ¼ļČĆļź╝ ļ¢Āļéś ļ╣äĻĄÉņĀü ļō£ļ¼╝Ļ▓ī ņ¦äļŻīņŚÉņä£ ļ¦īļéśĻ▓ī ļÉśļŖö ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļé£ņ▓ŁņØś ņ×äņāüņ¢æņāüĻ│╝ ņĖĪļæÉĻ│© CT ņåīĻ▓¼ņŚÉ ļīĆĒĢ£ ļ│Ė ņŚ░ĻĄ¼ņØś ļČäņäØ Ļ▓░Ļ│╝ļŖö ņČöĒøä ņ¦äļŻī ļ░®Ē¢ź Ļ▓░ņĀĢņŚÉ ļÅäņøĆņØ┤ ļÉĀ Ļ▓āņØ┤ļŗż.
Ļ▓░ļĪĀņĀüņ£╝ļĪ£, ņĀĢņāü Ļ│Āļ¦ēĻ│╝ ĻĖ░ļÅäĻ│©ļÅäņ░©ļź╝ Ļ░Ćņ¦ĆļŖö ļ╣äņÖĖņāüņä▒ ļé£ņ▓Ł ĒÖśņ×ÉņŚÉņä£ ņØ╝ņĖĪņä▒ņØ┤ ļŹö ĒØöĒĢśņśĆĻ│Ā ĒÅēĻĘĀ ĻĖ░ļÅäĻ│©ļÅäņ░©ļŖö 24.8┬▒10.3 dBļĪ£ ļéśĒāĆļé¼ļŗż. ņĖĪļæÉĻ│© CTņŚÉņä£ ļ╣äņĀĢņāüņåīĻ▓¼ļ│┤ļŗż ņĀĢņāü ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░Ļ░Ć ņĢĮĻ░ä ļŹö ļ¦ÄņĢśĻ│Ā, ņĖĪļæÉĻ│© CTņŚÉņä£ ļ╣äņĀĢņāü ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ņĀĢņāü ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ļ│┤ļŗż ņ¢┤ņØīļČäļ│äļĀźņØ┤ ņĀĆĒĢśļÉśņ¢┤ ņ׳ņŚłļŗż. ņłśņłĀņØä ĒåĄĒĢśņŚ¼ ņøÉņØĖņØ┤ ĒÖĢņØĖļÉ£ Ļ▓ĮņÜ░ļŖö ņØ┤Ļ▓ĮĒÖöņ”ØņØ┤ Ļ░Ćņן ĒØöĒĢśņśĆĻ│Ā ņĖĪļæÉĻ│© CT ļō▒ņØä ņØ┤ņÜ®ĒĢ£ ņ×äņāüņĀü ņ¦äļŗ©ņ£╝ļĪ£ļŖö ņ×Āļ│Ąņä▒ ņżæņØ┤ņŚ╝ņØ┤ Ļ░Ćņן ĒØöĒĢ£ ņøÉņØĖņØ┤ņŚłļŗż.