항암방사선 치료 후 대세포신경내분비암으로 전환된 상악동 편평세포암 1예
Abstract
Large cell neuroendocrine carcinoma (LCNEC) is a poorly differentiated neuroendocrine carcinoma that typically arises in the lung. Because of its rarity and poor prognosis, standardized treatment has not been established yet. A 53-year-old male was initially diagnosed as a maxillary sinus squamous cell carcinoma (SCC) arising from inverted papilloma (clinical stage of T4bN2bM0, stage IVb), and underwent concurrent chemoradiotherapy. After achieving complete remission for 3 years, recurrent tumors were found, of whom the pathologic diagnosis turned out to be LCNEC. He underwent endoscopic transnasal tumor extirpation, followed by adjuvant concurrent chemoradiotherapy. Until postoperative 12 months, he showed no evidence of recurrence. To the best of our knowledge, this is the first report of maxillary SCC transformed to LCNEC after chemoradiotherapy.
Key words: Carcinoma, neuroendocrine; ㆍ Cell transformation, neoplastic ㆍ Chemoradiotherapy ㆍ Maxillary sinus neoplasm ㆍ Papilloma, inverted
서 론
대세포신경내분비암(large cell neuroendocrine carcinoma, LCNEC)은 저분화(poorly differentiated) 신경내분비암(neuroendocrine carcinoma)으로, 예후가 매우 불량한 것으로 알려져 있다[ 1]. LCNEC는 매우 드문 유병률과 나쁜 예후로 인해 아직 표준 치료가 정립되어 있지 않으며, 일반적으로 환자 나이와 병변의 범위, 병기 등을 고려하여 다학제적 치료(multimodality treatment)를 시행하게 된다[ 2, 3]. 저자들은 상악동 편평세포암(squamous cell carcinoma, SCC)으로 항암방사선 치료 후 완전 관해를 이룬 후 3년만에 LCNEC로 전환되어 재발한 사례 1예를 치험한 바, 이를 문헌 고찰과 함께 보고하는 바이다.
증 례
53세 남성이 우측 상악에 임플란트 식립 후 4개월 뒤 농성 비루를 주소로 내원하였다. 비내시경상 우측 중비도에서 농성 비루를 동반한 종물이 확인되었으며( Fig. 1A and B) 외래에서 시행한 조직검사에서는 반전성 유두종으로 진단되었다. 부비동 자기공명영상(paranasal sinus magnetic resonance imaging, PNS MRI)을 촬영하였고, 조영증강이 되는 종물이 상악동 후벽과 외측벽을 파괴하고 각각 익구개와 공간과 측두하와 공간으로 침범하는 소견이 확인되었다( Fig. 1C and D). 악성종양이 동반되었을 것으로 판단하고 정확한 진단을 위해 전신마취하에 조직검사를 재시행하였고, 반전성 유두종에서 기원한 편평세포암(SCC)으로 진단되었다( Fig. 2). 경부림프절 전이도 확인되어 cT4bN2bM0 (stage IVb)의 병기 진단 하에 주 1회 cisplatin 투여를 포함한 항암방사선 치료(7000 cGy/35 fx)를 시행하였다. 방사선 치료는 세기조절 방사선 치료(intensity modulated radiation therapy, IMRT)로 시행하였다. 완전 관해 상태로 추적 관찰하던 중 항암방사선 치료 종료 후 3년이 되던 시점에 환자가 우측 유루증(epiphora) 및 비출혈 증상을 보였다. 비내시경상 우측 상악동 입구 및 하비갑개에 경계가 불명확한 종양이 확인되어 조직검사를 시행하였고, 대세포신경내분비암(LCNEC)으로 진단되었다. PNS MRI에서 우측 상악동에 조영증강되는 병변이 확인되었으며, 전방으로는 비루관(nasolacrimal duct), 후방으로는 익구개와 및 이관(eustachian tube)에 근접하는 양상이었으나 뚜렷한 침범 소견은 보이지 않았다( Fig. 3). 양전자방출단층 촬영(PET)에서 림프절 및 원격 전이는 없었으며, 전신마취하에 내시경적 내측상악절제술을 시행하였다. 종양학적 안전연 확보를 위해 이상구 직후방에 수직 절개를 넣어 점막 피판을 들어올린 뒤, 드릴과 골겸자 등을 이용하여 상악골의 전두돌기를 제거하여 비루관을 노출시켰다. 누낭의 직하부에서 비루관을 절제한 뒤 상악동 골점막을 상악골로부터 박리하고 상악 내측벽과 비강저의 경계에 절개선을 넣고 후방으로 연장하여 귀인두관융기(torus tubarius)의 전방 일부를 포함하여 비루관, 하비갑개, 상악골 내측벽 및 상악동 골점막을 종양 병변과 함께 일괴(en-bloc)로 절제하였다. 상악골 후벽 결손 부위를 통해 노출된 익구개와 부위에는 항암방사선치료 영향으로 인한 것으로 생각되는 연조직 유착 소견이 있어 추가로 제거하였다. 일괴로 절제된 병변의 전방 및 후방 절제연과 비루관 절제 부위에서 시행한 동결 절편 검사상 종양의 침범은 관찰되지 않았다. 조직검사 결과 LCNEC로 진단되었으며( Fig. 4), 전후방 절제연에서는 충분한 안전연이 확인되었으나 익구개와 부위에서 제거된 연조직에서 종양 세포의 국소 침범이 관찰되었다. SCC로 진단되었을 당시 LCNEC와 병발하였을 가능성을 고려하여 과거의 생검 조직 전체에 대해 면역조직화학염색을 포함한 추가 검사를 시행하였으나 초기 진단 당시 LCNEC에 부합하는 부분은 찾지 못하였으며, 모든 부위에서 SCC의 소견만 확인할 수 있었다( Fig. 2C- E). LCNEC의 불량한 예후와 익구개와 부위의 현미경적 미세 침범 소견을 고려하여 주 1회 cisplatin 투여를 포함한 항암 방사선치료(IMRT, 6000 cGy/30 fx)를 추가로 시행하였다. 현재 수술 후 12개월까지 조영증강 부비동 컴퓨터단층촬영(PNS contrast-enhanced CT) 및 내시경 검사에서 재발의 증거없이 외래 추적 관찰 중이다( Fig. 5).
고 찰
LCNEC는 매우 드물고 예후가 불량한 저분화 신경내분비암이다[ 4]. 두경부 영역에서 LCNEC는 후두에서 가장 많이 발생되며 이외 이하선, 비강 등에서 보고된 바 있다[ 1, 4, 5]. 국내에서 상악동에서 기원한 원발성 LCNEC 1예가 보고된 바 있으나, 본 증례와 같이 SCC에 대한 항암방사선 치료 후 LCNEC로 재발한 경우는 아직 보고된 바 없다[ 6]. 다른 기관의 경우 폐와 식도에서 SCC에서 LCNEC로 전환된 사례가 보고된 바 있다[ 7, 8]. 항암방사선 치료 후 SCC가 신경내분비 분화를 보이는 기전으로는 두 가지 가설이 제시되고 있다. 첫 번째는 신경내분비 분화를 보이는 종양 세포가 원래부터 존재한 상태에서 다른 세포보다 항암방사선 치료에 저항성을 보여 더 많은 비율로 잔존할 수 있다는 가설이다. 두 번째 가설은 원발종양에서는 신경내분비 분화가 없었으나 항암방사선 치료로 인한 세포 손상이 신경내분비 분화를 유도한다는 것이다[ 8]. 본 증례에서는 원발 종양에 대한 조직 슬라이드를 다시 광범위하게 조사해 봤지만 신경내분비 세포는 전혀 확인할 수 없었다. 물론 첫 치료시 종양을 완전 절제하여 조직검사를 시행하지는 않았으므로 원발 종양에 신경내분비 세포가 존재했을 가능성을 완전히 배제할 수는 없지만 적어도 획득한 조직 어디에서도 신경내분비 세포를 찾을 수 없었으며, 항암방사선 치료 후 3년간 완전 관해를 유지하다가 재발한 종양에서는 편평상피 부위가 확인되지 않는다는 점을 감안하면 두 가지 가설 중 후자의 가능성이 높을 것으로 생각된다. 비부비동 LCNEC의 임상 증상은 일측성 비부비동 종양에 의한 비출혈, 비폐색, 유루증, 안면통증 등이 있다[ 9]. 종양의 범위, 국소 침범 정도를 평가하기 위해 영상검사는 반드시 필요하나 영상검사로 LCNEC를 진단하기는 어렵다[ 6]. 병리조직학적 특징으로는 크기가 큰 세포에 상대적으로 작은 핵/세포질 비율, 많은 유사분열정도(>10/high-power field), 신경 내분비 분화도를 보이는 구조적인 패턴을 보이며, 면역조직화학염색에서 신경내분비 표지자인 synaptophysin, chromogranin, CD56에 양성을 보인다. 대세포와 소세포를 구분하는 특별한 표지자는 없고, 세포의 크기와 핵과 세포질 비 차이를 통해 감별할 수 있다[ 1, 4]. 비부비동 LCNEC는 매우 드물어서 표준 치료가 정립되어 있지 않으며, 예후가 매우 나쁘므로 다학제적 치료가 필요하다[ 2]. 메타분석 결과에 따르면 단독 요법으로 수술과 방사선 치료는 질병 특이 생존율 향상에 도움이 되나, 항암 치료는 생존율에 영향을 미치지 못하였다. 또한, 수술 후 방사선치료가 수술 단독 치료보다 생존율 향상에 이익이 있는 것으로 분석되었다[ 3]. 따라서 수술이 가능하다면 수술 후 방사선치료 또는 수술 후 항암방사선 치료가 타당하며, 수술로 완전 절제가 불가능할 시 항암방사선 치료를 고려하는 것이 타당할 것으로 생각된다[ 3, 6]. 이외 초치료를 시행함에도 재발하거나 전신 전이가 있을 경우, 제한적으로 면역억제제(immune checkpoint inhibitor, ICI)를 고려할 수 있으나 ICI의 뚜렷한 효과가 입증되지는 않았다[ 10, 11]. 본 증례는 반전성 유두종에서 유래된 편평세포암에 대한 항암방사선치료 후 재발암으로 LCNEC가 발생한 경우이다. LCNEC는 매우 예후가 불량한 것으로 알려져 있으나 저자들은 비내시경 접근법으로 종양을 완전 절제한 뒤 술 후 항암방사선 치료를 통해 12개월째까지 국소 재발 및 전신 전이의 증거 없이 추적 관찰 중으로 이를 문헌 고찰과 함께 보고하는 바이다.
ACKNOWLEDGMENTS
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2021R1A2C1013224).
Notes
Author contributions
Conceptualization: Sang-Wook Kim. Supervision: Sang-Wook Kim. Validation: all authors. Visualization: all authors. Writing—original draft: Sang-Wook Park, Sang-Wook Kim. Writing—review & editing: all authors.
Fig. 1.
Representative endoscopic and T1-weighted magnetic resonance images. A and B: Mass lesions with mucopurulent discharge are seen in the right middle meatus. C and D: Well-enhancing mass lesions in the right maxillary sinus exhibit the invasion into the pterygopalatine fossa (arrows; C) and the infratemporal fossa (arrowhead; D). 
Fig. 2.
Representative microscopic photographs. A: Endophytic growth of pseudostratified ciliated epithelium is seen in the main tumor, which is a characteristic of inverted papilloma (hematoxylin and eosin [H&E] staining, ×40). B: Invasion of dysplastic squamous cells with keratin pearls is seen, which indicates squamous cell carcinoma (H&E staining, ×200). C-E: In the immunohistochemical staining (×200), the specimen is positive for p40 (C), and negative for both CD56 (D) and synaptophysin (E). 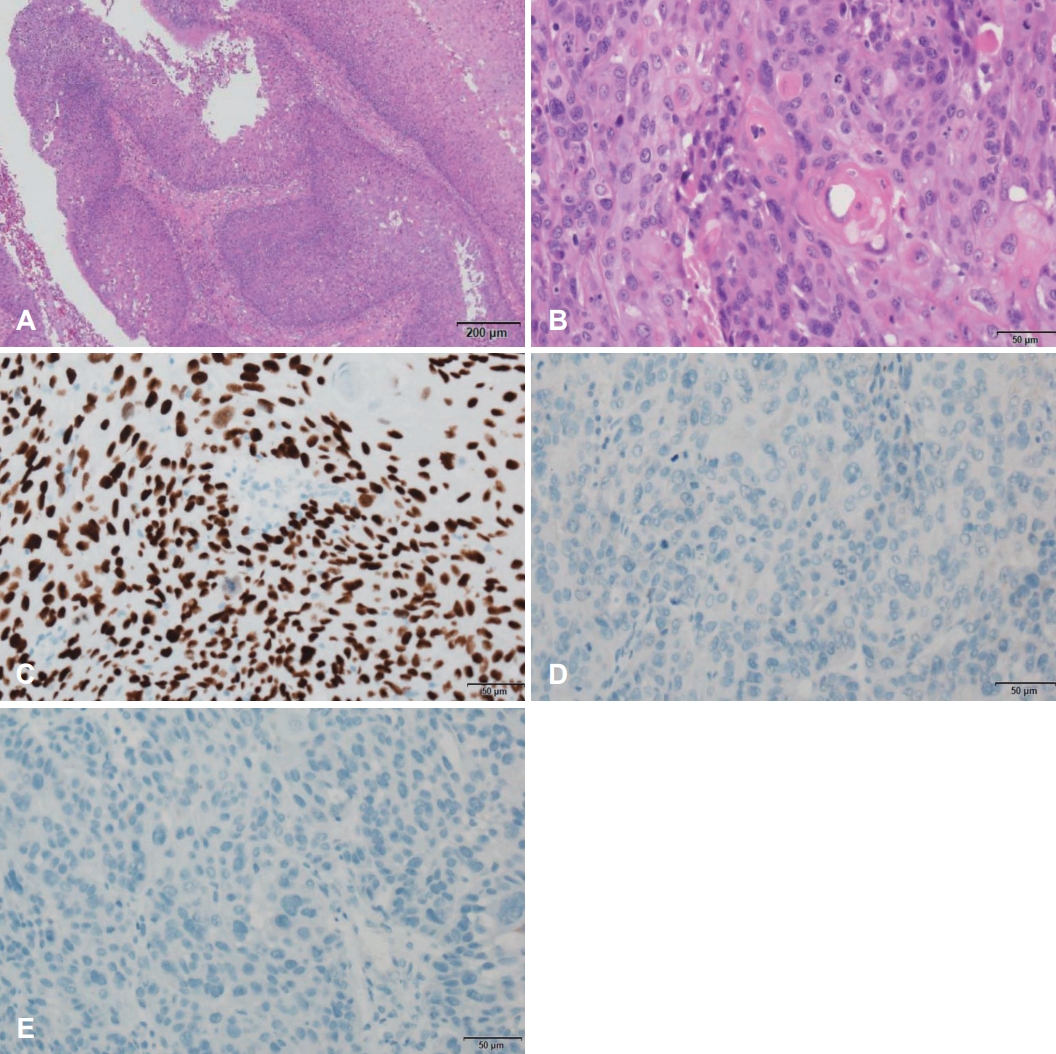
Fig. 3.
Representative T1-weighted paranasal sinus MR images. Well enhanced lesions (white arrows) are confined within the right maxillary sinus in the axial (A and B) and coronal (C) views. The lesions are adjacent to the nasolacrimal duct (white arrowhead) anteriorly (A), and the pterygopalatine fossa and the torus tubarius (yellow arrows) posteriorly (B), with no definite evidence of invasion. 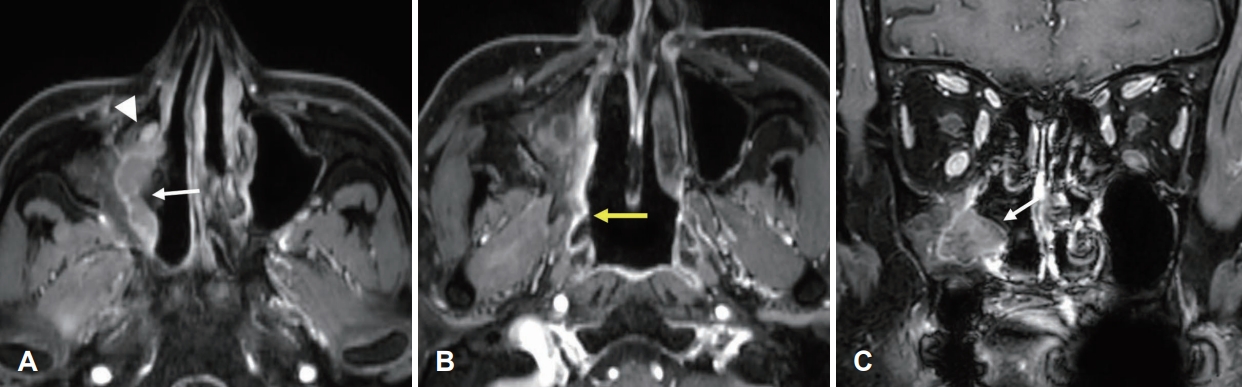
Fig. 4.
Representative histopathologic images of resected recurred tumors. A: Nests of atypical large cells with coarse nuclear chromatin, abundant cytoplasm and small nucleoli are observed, which are characteristics of large cell neuroendocrine carcinoma (hematoxylin and eosin staining, ×200). B-D: In the immunohistochemical staining (×200), the specimen is negative for p40 (B), and positive for both CD56 (C) and synaptophysin (D). 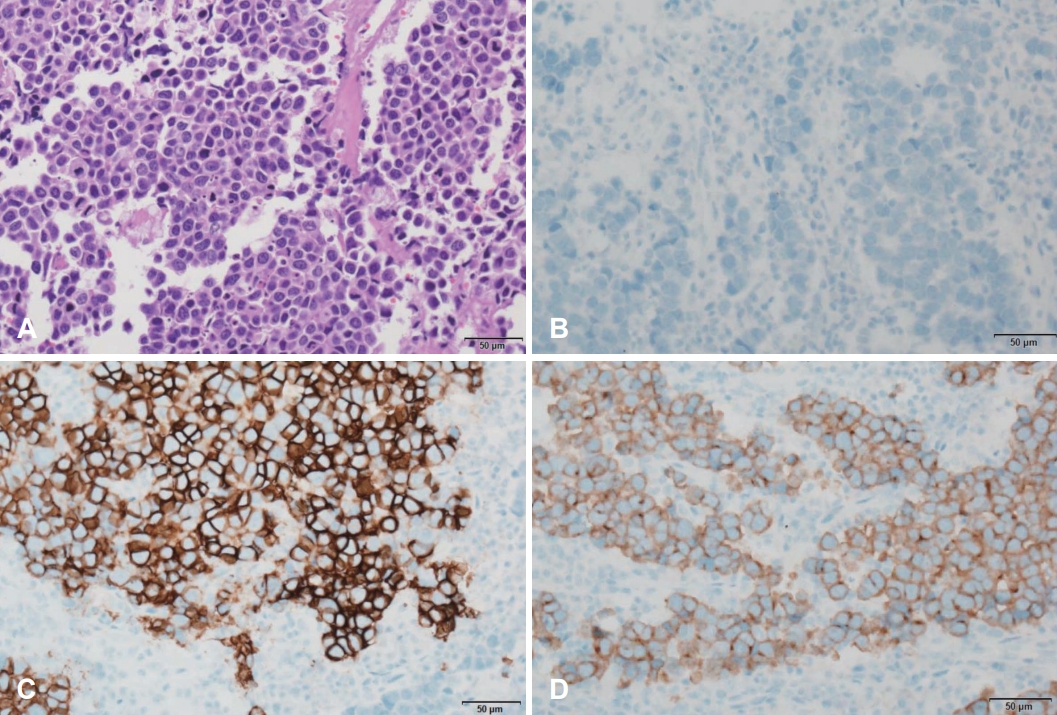
Fig. 5.
Postoperative 12-month endoscopic photographs and contrast-enhanced paranasal sinus CT images. A and B: The contracted right maxillary sinus (arrow) and crust formation over the pterygopalatine fossa area (asterisk) are seen with no evidence of tumor recurrence by 30°-angled rigid endoscopy. C and D: No enhanced lesions are observed in the axial (C) and coronal (D) CT images. 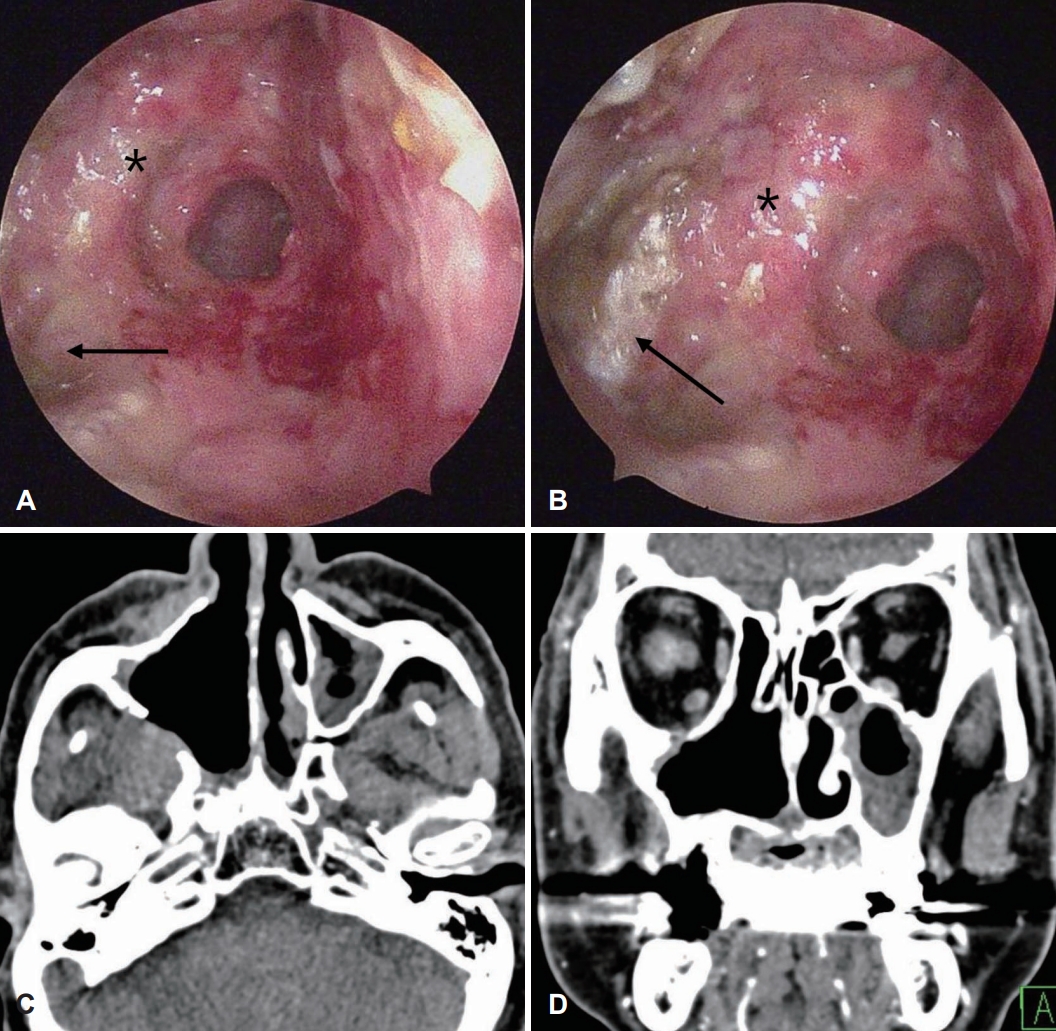
REFERENCES
1. WHO Classification of Tumours Editorial Board. WHO classification of tumours: head and neck tumours. 5th ed. Lyon: International Agency for Research on Cancer; 2022.
2. Patel TD, Vazquez A, Dubal PM, Baredes S, Liu JK, Eloy JA. Sinonasal neuroendocrine carcinoma: A population-based analysis of incidence and survival. Int Forum Allergy Rhinol 2015;5(5):448-53.   3. van der Laan TP, Iepsma R, Witjes MJ, van der Laan BF, Plaat BE, Halmos GB. Meta-analysis of 701 published cases of sinonasal neuroendocrine carcinoma: The importance of differentiation grade in determining treatment strategy. Oral Oncol 2016;63:1-9. 4. Kusafuka K, Ferlito A, Lewis JS Jr, Woolgar JA, Rinaldo A, Slootweg PJ, et al. Large cell neuroendocrine carcinoma of the head and neck. Oral Oncol 2012;48(3):211-5. 6. Lee YJ, Jeong JH, Oh YH, Ji YB. A case of large cell neuroendocrine carcinoma of the maxillary sinus. Korean J Head Neck Oncol 2019;35(2):45-9.  8. Morita M, Saeki H, Nakaji YU, Zaitsu Y, Hirahashi M, Ohguri T, et al. Conversion to neuroendocrine carcinoma from squamous cell carcinoma of the esophagus after definitive chemoradiotherapy. Anticancer Res 2016;36(8):4045-9. 10. Özdirik B, Jann H, Bischoff P, Fehrenbach U, Tacke F, Roderburg C, et al. PD-L1 - inhibitors in neuroendocrine neoplasia: Results from a real-life study. Medicine (Baltimore) 2021;100(1):e23835. 
|
|














