ņä£ ļĪĀ
ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ņØĆ ņāłņŚ┤ĻĖ░ĒśĢ, ļé£ņ▓Ł, ņŗĀņן ņØ┤ņāü ņåīĻ▓¼ ļō▒ņØ┤ ņ×äņāüņĀü ĒŖ╣ņ¦ĢņØĖ ņ¦łĒÖśņ£╝ļĪ£, ļīĆĻ░£ ņāüņŚ╝ņāēņ▓┤ ņÜ░ņä▒ ņ£ĀņĀäņØä ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ņ£Āļ│æļźĀņØĆ ņל ņĢīļĀżņĀĖ ņ׳ņ¦Ć ņĢŖņ£╝ļéś, Fraser ļō▒[1]ņØĆ 1980ļģäņŚÉ ņŗ¼ĒĢ£ ļé£ņ▓Ł ĒÖśņĢäņØś ņĢĮ 2%ņŚÉņä£ ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ņØä Ļ┤Ćņ░░ĒĢśņśĆĻ│Ā, 4ļ¦ī ļ¬ģļŗ╣ 1ļ¬ģņØś ņ£Āļ│æļźĀņØä ņČöņĀĢĒĢśņśĆļŗż. Ēæ£ĒśäĒśĢņØĆ ļŗżņ¢æĒĢśĻ▓ī ļéśĒāĆļéĀ ņłś ņ׳ņ£╝ļéś, ĒÖśņ×ÉņØś 90% ņØ┤ņāüņØ┤ ļé£ņ▓ŁņØä ļ│┤ņØ┤ļ®░, ņĀłļ░ś ņØ┤ņāüņŚÉņä£ ņĀ£2ĒśĢ ņāłņŚ┤ĻĖ░ĒśĢņØ┤ ļ│┤ņØ┤Ļ│Ā, 67% ņĀĢļÅäņŚÉņä£ ņŗĀņן ņØ┤ņāüņØä ļ│┤ņØ┤ļ®░, ĻĘĖ ņÖĖņØś ņ”Øņāüņ£╝ļĪ£ ņĀäņØ┤Ļ░£ ļłäĻ│Ą(53%), ņØ┤Ļ░£ ĻĖ░ĒśĢ(38%), ņÖĖņØ┤ļÅä Ēśæņ░®(12%)ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░Ļ░Ć ņ׳ļŗż[2]. ņ×äņāüņ¢æņāüņ£╝ļĪ£ ņ¢æņĖĪ ņĀ£2ĒśĢ ņāłņŚ┤ĻĖ░ĒśĢ ļ░Å ņÜ░ņĖĪ ņØ┤Ļ░£ ĻĖ░ĒśĢ(ņ£äņČĢ ĻĘĆ), ņ¢æņĖĪ ņĀäņØ┤Ļ░£ ļłäĻ│Ą, ņ¢æņĖĪ ļé£ņ▓Ł ļ░Å ņĀäĒśĢņĀüņØĖ Ļ░ĆņĪ▒ļĀźņØä ļ│┤ņØ┤ļŖö ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ ĒÖśņ×É 1ņśłļź╝ Ļ▓ĮĒŚśĒĢśņŚ¼ ļ¼ĖĒŚīĻ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”Ø ļĪĆ
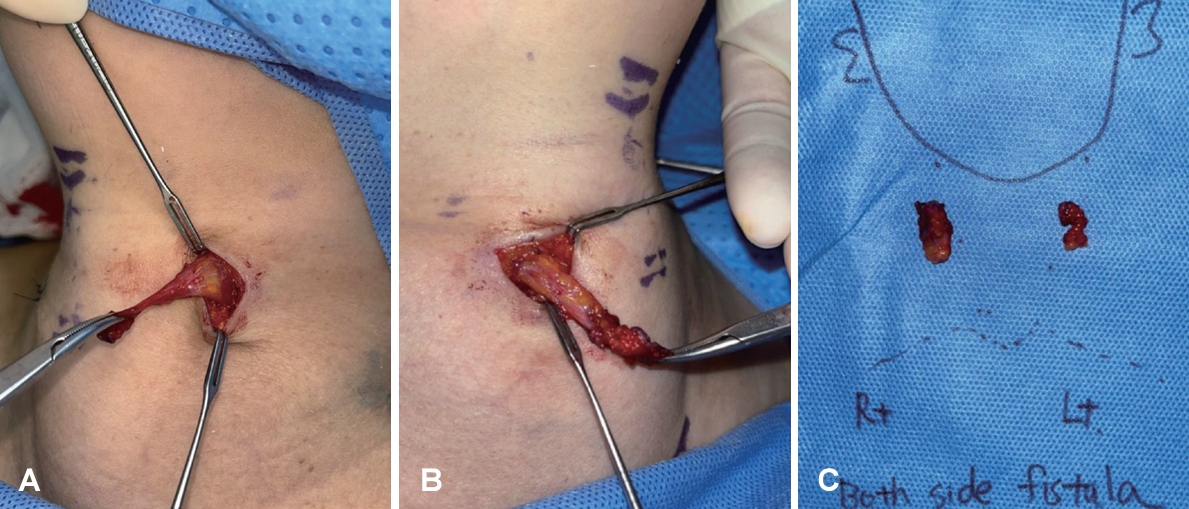
50ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉĻ░Ć ņÜ░ņĖĪ ņØ┤Ļ░£ ĻĖ░ĒśĢņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ņŗĀņ▓┤ Ļ▓Ćņ¦ä Ļ▓░Ļ│╝, ņäĀņ▓£ņä▒ ņ¢æņĖĪ Ļ▓ĮļČĆ ļłäĻ│Ą, ņ¢æņĖĪ ņĀäņØ┤Ļ░£ ļłäĻ│ĄņØä ļÅÖļ░śĒĢśĻ│Ā ņ׳ņŚłļŗż. ĒÖśņ×ÉļŖö ņ¢┤ļ”┤ņĀüļČĆĒä░ ņ¢æņĖĪ ļé£ņ▓ŁņØ┤ ņ׳ņŚłĻ│Ā, ņóīņĖĪ ļ│┤ņ▓ŁĻĖ░ļź╝ ņ░®ņÜ®ĒĢśĻ│Ā ņ׳ņŚłļŗż(Fig. 1). ņÜ░ņĖĪ ņØ┤Ļ░£ņä▒ĒśĢņłĀ, ņÜ░ņĖĪ ņĀäņØ┤Ļ░£ ļłäĻ│Ą ņĀłņĀ£ņłĀ ļ░Å ņ¢æņĖĪ Ļ▓ĮļČĆ ļłäĻ│Ą ņĀłņĀ£ņłĀņØä Ļ│äĒÜŹĒĢśņśĆļŗż. ņØ┤ĒĢÖņĀü Ļ▓Ćņé¼ņāü ņ¢æņĖĪ Ļ▓ĮļČĆ level 2ņŚÉ Ļ░üĻ░ü 1Ļ░£ņö® Ļ┤Ćņ░░ļÉ£ ļłäĻ│ĄņØĆ(Fig. 2A) ņóģļ¼╝ ļ░Å ļČäļ╣äļ¼╝ ņŚåņØ┤ ļČĆļō£ļ¤ĮĻ▓ī ņ┤ēņ¦ĆļÉśņŚłļŗż. ņ¢æņĖĪ ņØ┤Ļ░£ ņĢ×ņ¬Įņ£╝ļĪ£ Ļ┤Ćņ░░ļÉ£ ļłäĻ│Ą(Fig. 2B and C) ļśÉĒĢ£ ņóģļ¼╝ ļ░Å ļČäļ╣äļ¼╝ ņŚåņØ┤ ņ┤ēņ¦ĆļÉśņŚłļŗż. ņÜ░ņĖĪ ņØ┤Ļ░£ļŖö ņ£äņ¬Į 1/3 ļČĆļČäņØ┤ ņĢ×ņ£╝ļĪ£ ņĀæĒśĆ ņ׳ļŖö ņ£äņČĢĻĘĆ ņåīĻ▓¼ņØ┤ņŚłļŗż(Fig. 2D and E).
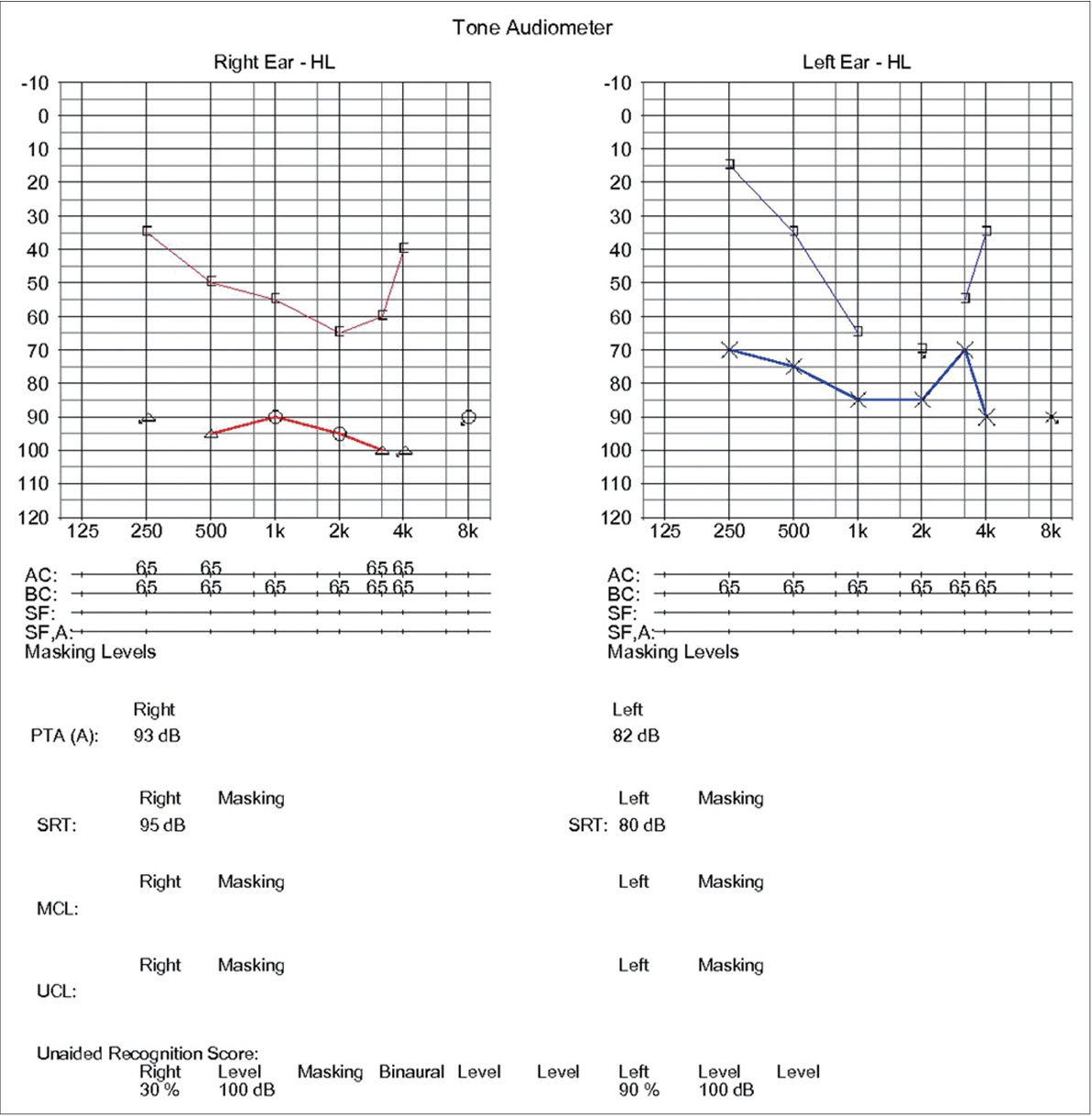
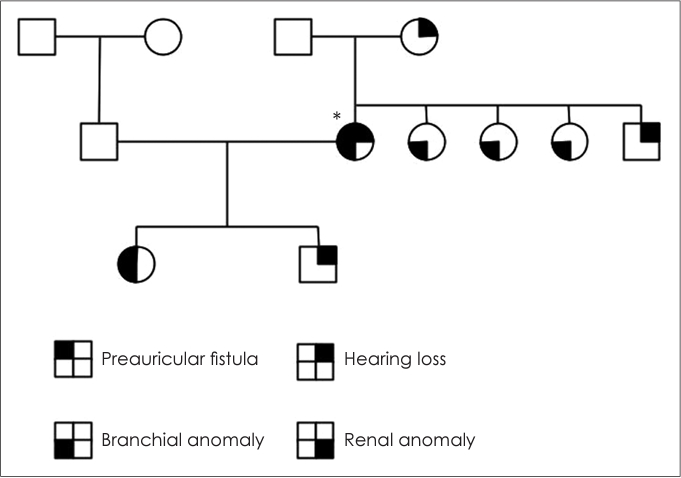
ņ×äņāüņĀü ņåīĻ▓¼ņ£╝ļĪ£ ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ ņØśņŗ¼ĒĢśņŚÉ Ļ░ĆņĪ▒ļĀźņŚÉ ļīĆĒĢ┤ņä£ ņĪ░ņé¼ĒĢśņśĆĻ│Ā, ņĀäĒśĢņĀüņØĖ ņāüņŚ╝ņāēņ▓┤ ņÜ░ņä▒ ņ¢æņāüņØä ļ│┤ņśĆļŗż. ņ¢┤ļ©ĖļŗłļŖö ņ¢æņĖĪ ļé£ņ▓ŁņØ┤ ņ׳ņŚłĻ│Ā, 3ļ¬ģņØś ņŚ¼ļÅÖņāØ ļ¬©ļæÉ Ļ▓ĮļČĆ ļłäĻ│ĄņØ┤ ņ׳ņŚłĻ│Ā ļé©ļÅÖņāØņØĆ ņóīņĖĪ ļé£ņ▓ŁņØ┤ ņ׳ņŚłļŗż. ĒÖśņ×ÉņØś ļöĖņØĆ ņ¢æņĖĪ ņĀ£2ĒśĢ ņāłņŚ┤ĻĖ░ĒśĢ, ņÜ░ņĖĪ ņĀäņØ┤Ļ░£ ļłäĻ│Ąņ£╝ļĪ£ ļ│ĖņøÉņŚÉņä£ ņłśņłĀĒĢśņśĆĻ│Ā, ņĢäļōżņØĆ ņ¢æņĖĪ ņżæņØ┤ņŚ╝ ļ░Å ņäĀņ▓£ņä▒ ņóīņĖĪ ļō▒Ļ│© Ļ│ĀņĀĢņ£╝ļĪ£ ļō▒Ļ│©ņĀłĻ░£ņłĀņØä ļ░øņĢśļŗż(Fig. 3).
Blood urea nitrogen, Ēü¼ļĀłņĢäĒŗ┤ņØä ĒżĒĢ©ĒĢ£ ĒśłņĢĪĻ▓Ćņé¼ ļ░Å ņåīļ│ĆĻ▓Ćņé¼ļŖö ņĀĢņāüņØ┤ņŚłĻ│Ā, ļ│ĄļČĆ CTņāüņŚÉņä£ ņ¢æņĖĪ ņŗĀņן ļ¬©ļæÉ ņĀĢņāüņØ┤ņŚłļŗż(Fig. 4A). ņĖĪļæÉĻ│© CTņŚÉņä£ ņØ┤ņåīĻ│© ņØ┤ņāüņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļéś, ņ¢æņĖĪ ņÖĆņÜ░ņØś ļČłņÖäņĀäĒĢ£ ĒÜīņĀä ļ░Å ņóīņĖĪ ņĀäņĀĢ ĻĖ░ĒśĢ ņåīĻ▓¼ņ£╝ļĪ£ ņ¢æņĖĪ ļé┤ņØ┤ ņØ┤ņāüņØä ļ│┤ņśĆļŗż(Fig. 4B-D).
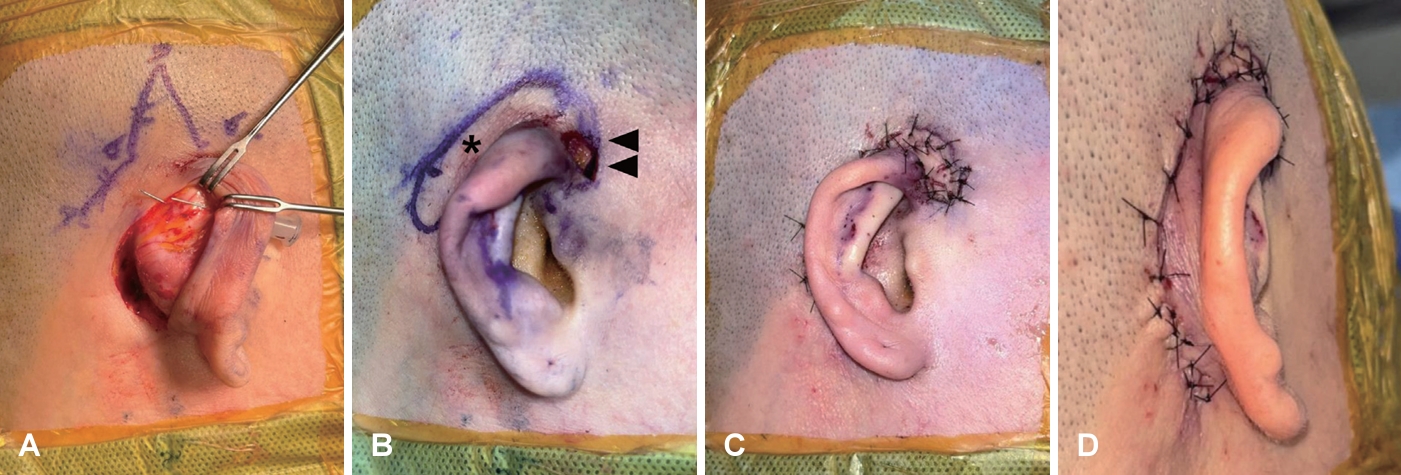
ņĀäņŗĀļ¦łņĘ©ĒĢśņŚÉ ņ¢æņĖĪ Ļ▓ĮļČĆ ņāłņŚ┤ļłäĻ│Ą ņŻ╝ņ£äļĪ£ ņĀłĻ░£ņäĀņØä ļäŻĻ│Ā, ļéŁņóģņØä ļö░ļØ╝ ĒīīņŚ┤ ņŚåņØ┤ ļ░Ģļ”¼ļź╝ ņ¦äĒ¢ēĒĢśņśĆļŗż. ļéŁņóģņØ┤ ļ¦╣Ļ┤ĆņØä ĒśĢņä▒ĒĢśĻ│Ā ņ׳ļŖö Ļ▓āņØä ĒÖĢņØĖĒĢ£ Ēøä ņ×¼ļ░£ņØś ņ£äĒŚśņØä ņżäņØ┤ĻĖ░ ņ£äĒĢ┤ ļ┤ēĒĢ® ļ░Å ļ¼ČņØīņØä ņŗ£Ē¢ēĒĢśņŚ¼ ļ¦łļ¼┤ļ”¼ĒĢśņśĆļŗż(Fig. 5). ņÜ░ņĖĪ ņĀäņØ┤Ļ░£ ļłäĻ│ĄņØĆ ņØ┤ļź£ ņŚ░Ļ│©(helical cartilage)Ļ│╝ ņĖĪļæÉĻĘ╝(temporalis muscle) ņØ╝ļČĆļź╝ ĒżĒĢ©ĒĢśņŚ¼ ņÖäņĀäĒ׳ ņĀ£Ļ▒░ĒĢśņśĆļŗż. ņÜ░ņĖĪ ņØ┤Ļ░£ ņä▒ĒśĢņłĀņØĆ ņØ┤ļź£ ņŚ░Ļ│©(helical cartilage)ņØś ņŚ░Ļ│©ļ¦ēņØä ļ░Ģļ”¼ĒĢśņŚ¼ ņŗ£ņ×æĒĢśņśĆļŗż. ņāüļČĆ ņØ┤Ļ░£ ņŚ░Ļ│©ņØś Ēøäļ░® ļé┤ņĖĪĻ│╝ ņÖĖņĖĪ ļæÉ ļ░®Ē¢źņŚÉ ņäØņāüļ┤ēĒĢ®(mattress suture)ņØä ĒĢśņŚ¼ ļīĆņØ┤ļź£ ņŻ╝ļ”ä(antihelical fold)ņØä ņāØņä▒ĒĢśļŖö ļ©ĖņŖżĒāĆļō£ ņłĀņŗØ(MustardeŌĆÖs suture)ņØä ĒĢśņśĆļŗż. ņØ┤Ēøä ņāüļ░®ņØś ļ¼╗ĒśĆņ¦ä ņØ┤ļź£ņ£╝ļĪ£ļČĆĒä░ ĒāĆņøÉĒśĢņØś Ēøäļ░® ņŚ░ņןņäĀņØä ļö░ļØ╝ ņĀłĻ░£ļź╝ Ļ░ĆĒĢśņŚ¼ Ēö╝ĒīÉņØä ļ¦īļōĀ ļÆż, Ēö╝ĒīÉņØä ņĀäļ░®ņ£╝ļĪ£ ĒÜīņĀäĒĢśņŚ¼ Ļ▓ĮĻ│äļź╝ ļ¦×ņČś Ēøä ļ┤ēĒĢ®ĒĢśļŖö V-Y ņĀäņ¦ä Ēö╝ĒīÉ(V-Y swing flap)ņØä ņŗ£Ē¢ēĒĢśņśĆļŗż(Fig. 6).
Ļ│Ā ņ░░
ņāłņŚ┤ņØ┤ņŗĀ ņ”ØĒøäĻĄ░ņØĆ ĒŖ╣ņ¦ĢņĀüņØĖ ņ”ØņāüņØä ļ░öĒāĢņ£╝ļĪ£ ņ¦äļŗ©ņØ┤ ņØ┤ļŻ©ņ¢┤ņ¦Ćļ®░ ņāłņŚ┤ĻĖ░ĒśĢ, ļé£ņ▓Ł, ņŗĀņן ņØ┤ņāü ņåīĻ▓¼ ļō▒ņØś ļŗżņ¢æĒĢ£ ņ×äņāüņĀü ĒŖ╣ņ¦ĢņØä ļ│┤ņØ┤ļŖö ņ¦łĒÖśņ£╝ļĪ£ ņŗĀņןņŚÉ ņØ┤ņāüņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ņØ┤ļØ╝Ļ│ĀļÅä ĒĢ£ļŗż[3]. ļīĆĻ░£ ņāüņŚ╝ņāēņ▓┤ ņÜ░ņä▒ ņ£ĀņĀäņØä ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳Ļ│Ā, ņøÉņØĖ ņ£ĀņĀäņ×ÉļĪ£ļŖö EYA1, SIX1, SIX5 ļō▒ņØ┤ ņĢīļĀżņĀĖ ņ׳ļŗż[4]. ĒŖ╣ņ¦ĢņĀüņØĖ ņ”Øņāü ņÖĖņŚÉļÅä ļō£ļ¼╝Ļ▓ī ĒĢśņĢģĒøäĒć┤, ņĢłļ®┤ļ¦łļ╣ä, ĻĄ¼Ļ░£ņŚ┤, ļ¬®ņĀ¢Ļ░łļ”╝ņ”Ø, ņäĀņ▓£ņä▒ ņŗ¼ņן ņØ┤ņāü, ĒĢŁļ¼ĖĒÅÉņćäņ”Ø, ĒÖŹņ▒ä ņ£äņČĢ ļō▒ņØ┤ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż[2].
Ļ░Ćņן ĒØöĒĢ£ ņ”ØņāüņØĖ ļé£ņ▓ŁņØĆ ņĀäņØīņä▒, Ļ░ÉĻ░üņŗĀĻ▓Įņä▒, Ēś╝ĒĢ®ņä▒ņØś ļ¬©ļōĀ ņ£ĀĒśĢņØś ļé£ņ▓ŁņØ┤ Ļ┤Ćņ░░ļÉśļ®░, ĻĘĖņżæ Ēś╝ĒĢ®ņä▒ ļé£ņ▓ŁņØś ņ£ĀĒśĢņØ┤ Ļ░Ćņן ĒØöĒĢśļŗż[2]. ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ņØ┤ ņØśņŗ¼ļÉśļŖö Ļ▓ĮņÜ░ ļé£ņ▓ŁņØś ĒÖĢņØĖņØä ņ£äĒĢ┤ ņł£ņØīņ▓ŁļĀźĻ▓Ćņé¼, ņ¢┤ņØīņŚŁņ╣śĻ▓Ćņé¼, ņ¢┤ņØīļ¬ģļŻīļÅä Ļ▓Ćņé¼ ļō▒ņØä ĒżĒĢ©ĒĢśņŚ¼ ņĀäļ░śņĀüņØĖ ņ▓ŁĻ░üĒÅēĻ░ĆĻ░Ć ĒĢäņÜöĒĢśļ®░, ņŗżņĀ£ ļé£ņ▓ŁņØ┤ ĒÖĢņØĖļÉ£ Ļ▓ĮņÜ░ņŚÉļŖö ņĀäņØīņä▒ ļé£ņ▓ŁņØś ņøÉņØĖ ļśÉļŖö ļé┤ņØ┤ ĻĖ░ĒśĢņŚÉ ļīĆĒĢ┤ņä£ ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ£ ņĖĪļæÉĻ│© ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśüņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗż[5]. ļé£ņ▓ŁņØ┤ ņ¦äĒ¢ēĒĢśļŖö Ļ▓ĮņÜ░ļŖö Ļ▒░ņØś ņŚåņ£╝ļéś ņĀäņĀĢņłśļÅäĻ┤Ć ĒÖĢņןņ”ØņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņ¦äĒ¢ēņä▒ ļé£ņ▓ŁņØä ļ│┤ņØ╝ ņłś ņ׳ņ¢┤ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż[6]. ĒÖĢņØĖļÉ£ ļé£ņ▓ŁņØĆ ņ¢Ėņ¢┤ ļ░£ļŗ¼ņŚÉ ņśüĒ¢źņØä ņŻ╝ĻĖ░ ļĢīļ¼ĖņŚÉ ņĀĢļÅäņŚÉ ļö░ļØ╝ ļ│┤ņ▓ŁĻĖ░ ļ░Å ņłśņłĀņĀü ņ╣śļŻīņÖĆ Ļ░ÖņØĆ ļ╣ĀļźĖ ņ╣śļŻīņĀü Ļ░£ņ×ģņØ┤ ņżæņÜöĒĢśļŗż.
ņØ┤Ļ░£ ĻĖ░ĒśĢņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ ĻĖ░ĒśĢņØś ņóģļźśņŚÉ ļö░ļźĖ ņ╣śļŻīļź╝ ĒĢśĻ▓ī ļÉ£ļŗż. ļ│Ė ĒÖśņ×ÉļŖö ņ£äņČĢĻĘĆ(constricted ear)ļź╝ ļ│┤ņśĆņ£╝ļ®░, ņØ┤ļŖö ņØ┤Ļ░£ņØś ņāüļČĆ 1/3ņŚÉ ĻĄŁĒĢ£ļÉ£ ņØ┤ļź£ ņŚ░Ļ│©ņØś ĻĖ░ĒśĢņØ┤ļŗż. Tanzer [7]ņØś 3Ļ░Ćņ¦Ć ļČäļźśņŚÉ ļö░ļź┤ļ®┤, ļ│Ė ĒÖśņ×ÉļŖö ņØ┤ļź£Ļ│╝ ņŻ╝ņāüņÖĆĻ░Ć ņĀæĒ׳Ļ│Ā ļīĆņØ┤ļź£Ļ│╝ ļīĆņØ┤ļź£Ļ░üņØ┤ ĒÄĖĒÅēĒĢ┤ņ¦ĆļŖö Ļ▓ĮņÜ░ļĪ£ ņØ┤ļź£ņØś ņ£äņČĢņØ┤ ņŗ¼ĒĢ£ ņżæ ļō▒ļÅäņØś 2ĒśĢ ĻĖ░ĒśĢņØä ļ│┤ņśĆļŗż. ņ£äņČĢĻĘĆņØś ņ╣śļŻīļŖö ĒĢ£ Ļ░Ćņ¦ĆņØś ņłĀņŗØļ¦īņ£╝ļĪ£ļŖö ļ¦īņĪ▒ņŖżļ¤¼ņÜ┤ Ļ▓░Ļ│╝ļź╝ ņ¢╗ĻĖ░ ņ¢┤ļĀżņÜ░ļ®░ ņØ┤Ļ░£ņØś ĒĢ┤ļČĆĒĢÖĻ│╝ ĻĖ░ĒśĢņØś ņĀĢļÅäņŚÉ ļö░ļØ╝ ļŗżņ¢æĒĢ£ ņłĀņŗØņØä ņĀüņÜ®ĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż[8]. Ļ▓ĮļÅäņżæļō▒ļÅäņØś ĻĖ░ĒśĢņŚÉņä£ļŖö Ļ╣āļ░£ Ēö╝ĒīÉļ▓Ģ(banner flap)ņØ┤ļéś Elsahy ņłĀņŗØ, ļ©ĖņŖżĒāĆļō£ ņłĀņŗØ, V-Y ņĀäņ¦ä Ēö╝ĒīÉ ļō▒ņŚÉ ņØśĒĢ£ ņØ┤ļź£ ĒÖĢņןņØä ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ņ£╝ļ®░[8], ļ│Ė ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ļ©ĖņŖżĒāĆļō£ ņłĀņŗØĻ│╝, V-Y ņĀäņ¦ä Ēö╝ĒīÉņØä ĒåĄĒĢśņŚ¼ ņ£äņČĢļÉ£ ņØ┤ļź£ņØś ĒÖĢņן ļ░Å ĒøäņØ┤Ļ░£ĻĄ¼ļź╝ Ļ╣ŖĻ▓ī ĒśĢņä▒ĒĢśņŚ¼ ļ¦łņŖżĒü¼ļź╝ ņōĖ ņłś ņ׳ņØä ņĀĢļÅäņØś ĒśĢĒā£ļź╝ ņØ┤ļŻ©ņŚłļŗż.
ļ│Ė ņ”ØļĪĆļŖö ņ¢æņĖĪ ņĀ£2ņŚ┤ ņāłņŚ┤ĻĖ░ĒśĢ, ņÜ░ņĖĪ ņØ┤Ļ░£ ĻĖ░ĒśĢ, ņ¢æņĖĪ ņĀäņØ┤Ļ░£ ļłäĻ│Ą, ņ¢æņĖĪ ļé£ņ▓Ł ļ░Å ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ Ļ░ĆņĪ▒ļĀźņØä ļ│┤ņØ┤ļŖö ĒÖśņ×ÉļĪ£ ņ¦äļŗ©ĻĖ░ņżĆ[9]ņŚÉ ļö░ļØ╝ ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ņ£╝ļĪ£ ņ¦äļŗ© Ēøä ņ”ØņāüņŚÉ ļ¦×ņČ░ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņ¢æņĖĪ ņĀ£2ĒśĢ ņāłņŚ┤ĻĖ░ĒśĢĻ│╝ ņĀäņØ┤Ļ░£ ļłäĻ│ĄņØĆ ņĀłņĀ£ņłĀņØä ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, ņÜ░ņĖĪ ņ£äņČĢĻĘĆļŖö ņØ┤Ļ░£ ņä▒ĒśĢņłĀņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░ ņłśņłĀ Ēøä ņ×¼ļ░£ ļō▒ņØś ņ¦ĢĒøä ņŚåņØ┤ ņ”ØņāüĒśĖņĀäņØä ļ│┤ņśĆļŗż. ņ¦ĆĻĖłĻ╣īņ¦Ć ĻĄŁļé┤ņŚÉņä£ļŖö ņ┤Ø 6ņśłņØś ņāłņŚ┤ņØ┤ ņ”ØĒøäĻĄ░ņØ┤ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░(Table 1) [10-15], ļ│Ė ņ”ØļĪĆļŖö ņØ┤Ļ░£ ĻĖ░ĒśĢņØä ļÅÖļ░śĒĢ£ ĒÖśņ×ÉņŚÉ ļīĆĒĢ┤ ņØ┤Ļ░£ ņä▒ĒśĢņłĀĻ│╝ ņ¢æņĖĪ ņāłņŚ┤ĻĖ░ĒśĢņØä ļÅÖļ░ś ņłśņłĀĒĢ£ ĻĄŁļé┤ ņ▓½ ņ”ØļĪĆļĪ£ņŹ© ņØśņØśĻ░Ć ņ׳ļŗż.