인후두 역류 질환 환자에서 타액 내 펩신 검출을 위한 타액 수집방법의 비교
Comparison of Methods for Collecting Saliva for Pepsin Detection in Patients with Laryngopharyngeal Reflux
Article information
Trans Abstract
Background and Objectives
To compare the simple spitting method and the Salivette® method of collecting saliva for detecting pepsin in patients with laryngopharyngeal reflux disease (LPRD).
Subjects and Method
Thirty-two patients diagnosed with LPRD by 24 hour multichannel intraluminal impedance and pH monitoring were enrolled prospectively. The amounts of pepsin in saliva determined by the simple spitting method and the Salivette® method were compared.
Results
Simple spitting showed higher sensitivity, specificity, accuracy, positive predictive value and negative predictive value. There was no statistically significant difference between the amount of pepsin detected by simple spitting (10.07±11.68 ng/mL) versus that detected using the Salivette® method (7.09±7.27 ng/mL) (p=0.258).
Conclusions
The simple spitting method has higher sensitivity, specificity and accuracy than the Salivette® method for detecting pepsin in patients with LPRD.
Introduction
Laryngopharyngeal reflux disease (LPRD) is defined as the reflux of gastric content to the pharynx and larynx [1]. Until recently, diagnosis of LPRD has been difficult and controversial [2]. Laryngoscopic findings, especially edema and erythema, are often used to diagnose LPRD by otolaryngologist. However, it has been demonstrated that accurate clinical assessment of LPRD using these findings is likely to be difficult because laryngeal physical findings exhibit high inter-clinician variability, which makes the precise laryngoscopic diagnosis of LPRD highly subjective [3]. Multichannel intraluminal impedance and pH (MII-pH) monitoring seem to show better performance in diagnosing extraesophageal manifestations of gastroesophageal reflux disease (GERD), thanks to their ability to evaluate acid and nonacid refluxes other than their proximal extensions [4].
Several recent studies have investigated the potential use of pepsin as a diagnostic marker for LPRD [5-8]. After exposure of laryngeal mucus to the stomach contents, which contain acid and pepsin, pepsin activity depletes the level of carbonic anhydrase III. This depletion inhibits the expression of the protective mucins 2, 3, 5A, 5B, Sep70, and Sep53, in addition to that of E-cadherin. These proteins play a vital role in maintaining cellular integrity of the epithelium [9].
Despite the clear importance of pepsin, no formal method of collecting saliva has yet been validated to detect pepsin in patients with LPRD. The aim of this study was to identify the best method of collecting saliva to detect pepsin in patients with LPRD by comparing the simple splitting method and the relatively new Salivette® method.
Subjects and Method
Subjects and study design
This study prospectively evaluated 35 patients who underwent 24 hour MII-pH monitoring for a chief complaint of LPRD symptoms such as globus sensation, hoarseness, or chronic cough. Patients with a history of any esophageal or gastric surgery or previously diagnosed with LPRD were excluded. Before starting the test, patients completed a survey to assess their subjective symptoms (reflux symptom index, RSI) and health-related quality of life (HRQoL). In addition, laryngeal examinations were performed to objectively assess the finding reflux finding score (RFS). The method of this study provided sufficient explanation to the patients and the patients’ consent was obtained. This study was approved by our Institutional Review Board (IRB No. 2014-09-201).
Simple spitting /Salivette®
Subjects were asked to collect the early morning sample before eating or drinking and before brushing their teeth. For this sample, patients were instructed to collect saliva by simple spitting after a throat clearing maneuver and by using the Salivette® apparatus. Saliva was obtained using the Salivette® as follows: First, the patient removes the swab from the Salivette®, places the swab in the mouth, and chews the swab for about 60 seconds to stimulate salivation (Fig. 1). Next, the patient returns the swab with the absorbed saliva to the Salivette® and replaces the stopper. Simple spitting and Salivette® were performed in same day, and the patients were randomly selected without giving any advance notice. After collection, the sample is returned to the inspector. All saliva samples were collected in conical tubes and were spun by centrifugation for 2 minutes at 1000 g. Particles and mucus strands were thus collected in the extended tip of the tube. The closed insert containing the swab was then hygienically disposed of. The recovered saliva was used for pepsin detection.
Salivette® to collect saliva samples for measurement of pepsin.
We used 30 mL collection tubes containing 0.5 mL 0.01 M citric acid (pH 2.5), a pepsin-stabilizing agent. Samples were refrigerated at -80℃ and analyzed within 2 months of collection. Saliva samples were centrifuged at 1000 g for 15 min at 4℃, and the supernatants were harvested.
We determined pepsin levels in saliva samples using a pepsin enzyme-linked immune-sorbent assay (ELISA) kit (Cloud-Clone, Houston, TX, USA). Briefly, saliva was added to a percolated 96-well plate, detection reagent A was immediately added, and the plate was incubated for 1 hour at 37℃. The wells were washed and incubated with detection reagent B for 30 minutes at 37℃. The wells were then washed and incubated with TMB Substrate solution for 15 minutes at 37℃. The reaction was stopped using Stop Solution, and the absorbance of each sample was immediately evaluated at 450 nm using a microplate reader. The assays were interpreted by a single investigator blinded to both the patient’s clinical status and questionnaire results.
24 hour MII-pH monitoring
The dual-channel MII-pH catheter used in this study was composed of a 2.3-mm polyurethane catheter that incorporated six impedance segments and two pH-measuring electrodes (ZepHr-Impedance/pH Reflux Monitoring System; Sandhill Scientific Inc., Highlands Ranch, CO, USA). The catheter models (ZAI-BL-54, 55, 56, Comfor-TEC Z/PH single- use probe with 2.3-mm diameter; Sandhill Scientific, Inc.) used were based on the patient’s esophageal length. The configuration of this catheter enabled recording of changes in the intraluminal impedance at each point. Additionally, pH was monitored at the hypopharynx (proximal, pH 1) and esophagus (distal, pH 8). Using direct visualization, a fiberoptic scope was inserted into the nasal cavity to assist probe placement. A dual-channel MII-pH catheter was then inserted through the nose to the opposite side of the fiberscope inserted before, and the blue visualization band was placed 1 cm below the proximal pH sensor at the proximal edge of the upper esophageal sphincter [10].
The probe was attached to an external electronic data recorder for 24 hours in order to monitor esophageal pH. The probe was removed the following day, and the pH data was downloaded for analysis (ZepHr CompactFlash Card and Recorder; Sahnhill Scientific Inc.). Patients were instructed to record the time of each meal and to document the occurrence of cough, globus, heartburn, or regurgitation [11].
We chose three MII parameters to evaluate: 1) number of nonacid reflux events that reached the proximal esophagus, 2) number of acid reflux events that reached the proximal esophagus, and 3) number of total reflux events that reached the proximal esophagus.
A minimum of 1 event of LPRD was judged to be indicative of LPRD.
Statistical analysis
All statistical analyses were performed using SPSS 18.0 software (SPSS Inc., Chicago, IL, USA). To identify the best method for saliva collection to detect pepsin, the Wilcoxon signed rank test was used. Agreement ratios were evaluated using the chi-square test. A p-value<0.05 was considered statistically significant.
Results
Thirty-two subjects were diagnosed with LPRD and three subjects were diagnosed as normal by 24 hr MII monitoring. The subjects with LPRD consisted of 21 (65.6%) women and 11 (34.4%) men. The mean patient age was 50.0±14.9 years and the number of mean LPRD events by MII monitoring was 5.41±4.61. Evaluation of subjective symptoms showed that the mean RSI was 15.06±5.17 and the mean HRQoL was 73.09±49.67. With respect to objective findings, the mean RFS value was 10.84±3.38 (Table 1).

Baseline demographic and clinical characteristics of patients with LPRD
For diagnostic test evaluation, the agreement ratio between the MII result and the presence of pepsin in saliva according to each method (simple spitting and Salivette®) was analyzed. The simple spitting method showed higher results in all five categories (sensitivity, specificity, accuracy, positive predictive value, and negative predictive value) (Table 2).
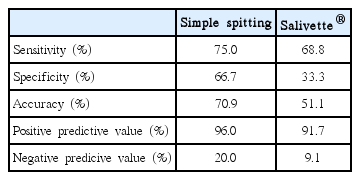
Agreement ratios between detection of pepsin in saliva and multichannel intraluminal impedance and pH monitoring
In comparison of detecting pepsin level between two methods, the simple spitting method yielded a higher pepsin level than the Salivette® method, although this difference was not statistically significant (10.07±11.68 ng/mL vs. 7.09±7.27 ng/mL, p=0.258).
Discussion
Symptoms of LPRD are commonly seen in ENT clinics [12], and the prevalence of LPRD is increasing [13]. However, no established definition has yet been validated for the diagnosis of LPRD. Laryngoscopic findings, especially edema and erythema, are often used to diagnose LPRD by ENT surgeons [14]. However, it has been demonstrated that accurate clinical assessment of LPRD is likely to be difficult because laryngeal physical findings exhibit high inter-clinician variability, which makes the precise laryngoscopic diagnosis of LPRD highly subjective [3].
MII-pH monitoring seems to show better performance in diagnosing extra-esophageal manifestations of GERD, due to its ability to evaluate acid and nonacid refluxes other than their proximal extensions [4,15-17]. Currently, 24 hour MII-pH monitoring is believed to be the most accurate diagnostic tool. However, this method is relatively invasive for patients, time-consuming, and costly.
A number of studies have attempted to define methods for diagnosing LPRD. In these studies, interest has increased in the role of pepsin, which is responsible for the development of mucus injury to the laryngopharynx [2,18]. Since pepsin (like acid) is made only in the stomach, it may be a good marker for laryngeal reflux. Thus, the identification of pepsin in the larynx may be a suitable proxy for reflux of gastric contents [19]. In addition, collecting pepsin provides a convenient, office-based, noninvasive, quick, and inexpensive technique that is different from the other available diagnostic tools [20].
Because few studies have focused on developing and validating methods for detecting pepsin [18,21], the authors paid attention to the method of collecting saliva for detecting pepsin. Specifically, we compared the simple spitting and Salivette® methods of detecting pepsin. The advantages of the Salivette® collection over spitting into a tube are a simple and hygienic collection, decreased viscosity of the saliva and removal of dead cells, glycoproteins and other subcellular substances. It is noteworthy that Salivette® is an important collection tool, especially when obtaining saliva is restricted, as in procedures involving newborns or during intense exercise conditions. We found that the amounts of pepsin detected by the two methods were not significantly different. We next evaluated the agreement ratio between MII results and the presence of pepsin in saliva and found that the simple spitting method had superior sensitivity and a superior negative predictive value. Thus, our results do not identify any advantage of the Salivette® method for detecting pepsin in saliva. The simple spitting method can collect the saliva from the pharynx, while the Salivette® method absorbs the saliva that emerges during chewing. This seems to show the difference in the results.
One previous study found that the pepsin amount, as obtained through a throat clearing maneuver within four hours of the participant’s last meal, was positively correlated with one RFS item, specifically ventricular obliteration. However, no significant differences were observed with respect to the other RFS components except ventricular obliteration between different pepsin values [22]. Several methods for collecting saliva are possible, and other approaches for detecting pepsin are also possible. It is conceivable that the obtained pepsin value will vary according to the detection method; thus, it is important to find the most appropriate value in the context of LPRD diagnosis. This is the first trial to compare the abilities of different methods to detect pepsin.
In conclusion, the simple spitting method had higher sensitivity than the Salivette® method for detecting pepsin in patients with LPRD.
Acknowledgements
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) & funded by the Korean government (MSIP & MOHW) (NRF-2015M3A9E2029189).