돌발성 난청 환자에서 전신 스테로이드 단독요법과 고실 내 스테로이드 병용요법의 치료 효과 비교
Comparison of Hearing Outcomes of Systemic Steroid Monotherapy and Intratympanic Steroid Combined Treatment in Idiopathic Sudden Sensorineural Hearing Loss
Article information

Trans Abstract
Background and Objectives
Steroid treatment is used as a main treatment modality for sudden sensorineural hearing loss (SSNHL). Intratympanic injection of steroid (ITS) has been used and its therapeutic efficacy reported as being comparable to the systemic steroid administration (SS). This study compares the hearing outcomes of using ITS and SS simultaneously and SS alone.
Subjects and Method
Retrospective chart review was performed for 146 patients with SSNHL. The patients were divided into 2 groups according to the method of treatment (SS and ITS simultaneously vs. SS alone). The inclusion criteria were starting treatment within 7 days after onset, and follow up pure tone audiometry at least 4 weeks after treatment. Hearing gain for pure tone threshold of each frequency and average of 4 frequencies (500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz) were compared between both groups.
Results
The improvement in PTA at 1-month follow-up was 27.3±20.0 dB HL in the simultaneous group and 19.1±19.5 dB HL in the SS alone group; this was not statistically significant. Complete or partial recovery at 1-month follow-up was observed in 65.3% of the simultaneous group and 69.6% of the SS alone group; this was also not significant.
Conclusion
There was no significant difference in hearing outcomes between the simultaneous and SS alone group. The simultaneous therapy does not appear to be superior to the SS alone therapy. Further studies using more population and longer follow-up periods are necessary.
서 론
돌발성 난청은 갑작스러운 청력 저하가 발생하는 질환으로, 72시간 내에 3개 이상의 연속된 주파수에서 30 dB 이상의 감각신경성 청력 저하가 나타나는 것으로 정의한다[1]. 치료 시기가 늦어질 경우 청력 예후가 불량할 수 있으며, 환자의 삶의 질이 저하될 수 있기 때문에 즉각적인 진단과 치료가 필요하다[2,3]. 돌발성 감각신경성 난청의 일차 치료법으로 전신적 스테로이드 치료와 고실 내 스테로이드 주입술이 사용되고 있으며, 두 가지 치료 모두 효과가 비슷한 것으로 알려져 있다[4-8]. 전신적 스테로이드 치료와 고실 내 스테로이드 주입술을 동시에 시행하는 것과 전신적 스테로이드 치료 단독요법을 비교했을 때, 병합요법이 더 좋은 청력 회복을 보인다는 결과가 다수 보고되었다[9-13]. 하지만 고실 내 스테로이드 주입을 동시에 시행했을 때 추가적인 이득이 없다는 연구 결과도 있다[14-16]. 따라서 본 연구는 전신적 스테로이드 단독 치료와 고실 내 스테로이드를 병행하였을 때의 청력 회복 정도를 비교해 보고자 한다.
대상 및 방법
2015년 1월~2017년 12월까지 본원 이비인후과에서 돌발성 난청 진단하에 치료를 받은 환자를 대상으로 후향적 의무기록 분석을 하였다. 대상 환자의 선정 기준은 뚜렷한 원인 없이 3일 이내에 순음청력검사상 3개의 연속되는 주파수에서 30 dB 이상의 감각신경성 난청 소견을 보이는 환자 중 발병 후 1주 이내에 치료를 시작한 환자로 하였다. 이 중 10 dB 이상의 전음성 난청이 있는 환자, 뇌 병변 혹은 외상에 의한 난청 환자, 메니에르병 및 중이염의 과거력이 있는 환자는 분석 대상에서 제외하였다. 총 146명이 위 조건에 부합하였으며, 이 중 경구 스테로이드제와 고실 내 스테로이드 주입술을 병행하여 시행한 군을 A군, 경구 스테로이드제만 투약한 군을 B군으로 나누었다.
두 군 모두 prednisolone(SolondoⓇ, Yuhan Corp., Seoul, Korea)을 제1일에서 제5일까지 환자 개별 몸무게에 따라 하루 1 kg당 1 mL의 용량으로 오전, 오후 총 2회로 경구 분복 투여하였고, 최대 하루 80 mg을 초과하지 않도록 하였다. 제6, 7일에 용량을 절반으로 줄여서 투약하였고, 제8, 9일에 오전 10 mg, 오후 10 mg으로 총 20 mg를 분복 투여하였고, 제10일에 하루 총 10 mg 투여하여, 총 10일간 투여하였다. 고실 내 스테로이드 주입술은 dexamethasone(Dexamethasone phosphate disodiumⓇ, 5 mg/mL, Huons Medical, Seoul, Korea)을 사용하였고, 2일 간격으로 최소 3회 이상 시행하였으며, 1 mL 투베르쿨린 시린지에 25 게이지 바늘을 부착하여 고막 전하방부에 주입하였고, 1회 주입량은 약 0.5 mL였다. 약물 주입 후 앙와위에서 주입한 반대 측으로 고개를 돌린채 30분 정도 유지시켰다.
청력 평가는 순음청력검사를 치료 시작 전 1회, 치료 시작 후 2주일째 1회, 치료 시작 후 1개월째 1회 시행하였으며, 각각의 청력역치 호전도에 따라 치료 효과를 판정하였다. 청력역치의 평균값은 0.5, 1, 2 및 4 kHz의 6분법으로 계산하였으며, 2012 AAO-HNSF Clinical Practice Guideline: Sudden Hearing Loss에 따라 치료 호전 여부를 판정하였다[17]. 치료 후 청력역치가 정상 측 순음청력역치의 10 dB 이내로 회복된 경우를 완전회복군(complete recovery), 치료 전 순음청력역치의 50% 이내로 회복되거나, 청력역치 호전도가 10 dB 이상인 경우를 부분회복군(partial recovery)으로 분류하였다. 부분회복군 중 청력이 50 dB 이하로 회복되는 경우 의미 있는 청력 회복으로 판정하였다. 또한, 청력역치 호전도가 10 dB 미만인 경우를 미회복군(no improvement)으로 분류하였다. 완전회복군 및 부분회복군을 모두 포함하여 청력 회복으로 간주하였을 때, 두 군 간 회복률의 차이가 나타나는지 비교하였다. 또한 A군 내에서 고실 내 스테로이드 주입술을 4회 이하로 시행한 군과 5회 이상 시행한 군을 별도로 구분하여 회복률 및 주파수별 호전 정도의 차이가 나타나는지 분석하였다.
통계적 분석은 SPSS 24.0(IBM Corp., Armonk, NY, USA)을 통해 t-검정 혹은 Mann-Whitney U test, 카이 제곱 분석 및 Fisher’s exact test를 시행하여 두 군을 비교하였다. p값이 0.05 이하인 경우에 유의한 차이가 있는 것으로 판정하였다. 각 자료의 평균은 중앙값과 표준편차로 표기하였다.
결 과
A군은 총 55명으로 평균 나이 53.8±14.5세, 남녀 성비는 26:29, 병변 방향은 우측과 좌측 비 27:28이었다. 발병 후 초기 치료까지의 기간은 평균 3.1±2.1일이었으며, 어지럼이 있는 경우는 11명(20%), 이명이 있는 경우는 26명(47.2%)이었다. 6분법상 초기 순음청력역치의 평균은 68.2±23.5 dB, 순음청력검사 패턴에 따라 상승형 7명(12.7%), 편평형 25명(45.4%), 하강형 23명(48.2%)이었다. 당뇨가 있는 환자는 6명(10.9%), 고혈압이 있는 환자는 14명(25.4%)이었고, 고실 내 스테로이드 주입술 평균 시행 횟수는 5.5±2.2회였다. B군은 총 91명으로 평균 나이 51.5±14.8세, 남녀 성비는 54:47, 병변 방향은 우측과 좌측 비 45:46이었다. 발병 후 초기 치료까지의 기간은 평균 2.9±2.2일이었으며, 어지럼이 있는 경우는 24명(26.3%), 이명이 있는 경우는 62명(68.1%), 6분법상 초기 순음청력역치의 평균은 55.9±25.5 dB, 순음청력검사 패턴에 따라 상승형 29명(31.8%), 편평형 21명(23.0%), 하강형 41명(45.0%)이었다. 당뇨가 있는 환자는 10명(10.9%), 고혈압이 있는 환자는 23명(25.2%)이었다. 양 군 사이의 연령, 성별, 병변 방향, 발병 후 초기치료까지의 기간, 초기 순음청력역치, 초기 어지럼 또는 이명 동반 유무, 당뇨 또는 고혈압 동반 유무에 대해 카이 제곱 검정 및 t-검정을 시행하였다. A군의 치료 전 순음청력역치가 B군에 비해 유의하게 높았으며(p<0.05), 이외의 다른 요인들은 유의한 통계학적 차이는 없었다(Table 1).
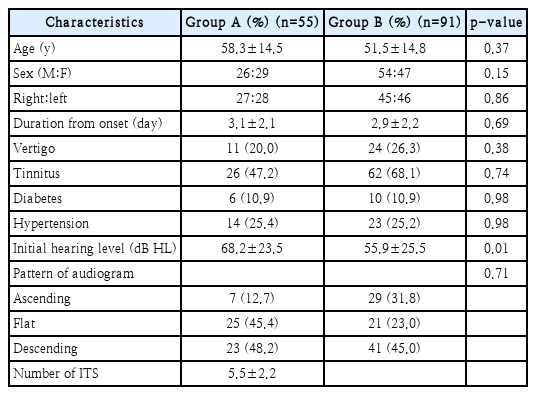
Subject demographic data
2주 치료 후 청력 호전 비교
청력역치 호전도는 A군은 22.6±23.4 dB, B군은 17.2±19.6 dB로 양 군 간의 유의미한 통계학적 차이는 없었다(p>0.05) (Fig. 1A). 각 주파수별 청력역치 호전도를 양 군간 비교하였을 때, 유의미한 차이는 없었다(p>0.05)(Fig. 2A).

Comparison of hearing gain between simultaneous SS with ITS and SS alone. There was no significant difference in hearing gain between the two groups after 2 weeks (p>0.05) (A). There was no significant difference in hearing gain between the two groups after 1 month of treatment (p>0.05) (B). ns: not significant, SS: systemic steroid administration, ITS: intratympanic injection of steroid.

Hearing gain for each frequency at post-treatment 2 weeks and 1 month. There was no significant difference in hearing gain for each frequency between the two groups after 2 weeks (p>0.05) (A). There was no significant difference in hearing gain for each frequency between the two groups after 1 month of treatment (p>0.05) (B). ns: not significant.
치료 2주 후 회복 정도를 2012 AAO-HNSF Clinical Practice Guideline에 따라 비교했을 때, A군에서 완전회복을 보인 경우는 20명(36.3%), 유의미한 부분회복을 보인 경우는 10명(18.1%), 무의미한 부분회복을 보인 경우는 6명(10.9%)이었고, 회복이 없는 경우는 19명(34.5%)이었다. B군에서 완전회복을 보인 경우는 48명(52.7%), 유의미한 부분회복을 보인 경우는 6명(6.6%), 무의미한 부분회복을 보인 경우는 4명(4.4%)이었고, 회복이 없는 경우는 33명(36.2%)이었다. 완전회복군과 부분회복군을 청력 회복으로 간주하여 양 군 간의 회복률의 차이를 카이 제곱 검정하였을 때, A군은 36명(65.3%), B군은 58명(63.7%)으로 유의미한 통계학적 차이는 없었다(p>0.05)(Table 2).
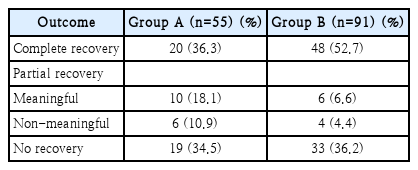
Hearing recovery after 2 weeks
1개월 치료 후 청력 호전 비교
청력역치 호전도는 A군은 27.3±20.0 dB, B군은 19.1±19.5 dB로 양 군 간의 유의미한 통계학적 차이는 없었다(p>0.05) (Fig. 1B). 각 주파수별 청력역치 호전도를 양 군간 비교하였을 때, 유의미한 통계학적 차이는 없었다(p>0.05)(Fig. 2B). 치료 1개월 후 청력 회복 정도를 2012 AAO-HNSF Clinical Practice Guideline에 따라 비교하였을 때, A군에서 완전회복을 보인 경우는 13명(38.2%), 부분회복을 보인 경우는 7명(20.5%)로 모두 유의미한 부분회복을 보였고, 회복이 없는 경우는 14명(41.1%)이었다. B군은 총 44명 중 완전회복을 보인 경우는 6명(13.6%), 유의미한 부분회복을 보인 경우는 18명(40.9%), 무의미한 부분회복을 보인 경우는 5명(11.3%)이었고, 회복이 없는 경우는 15명(36.2%)이었다. 완전회복군과 부분회복군을 청력 회복으로 간주하여 양 군 간의 회복률의 차이를 카이 제곱 검정하였을 때, 유의미한 통계학적 차이는 없었다(p>0.05)(Table 3).
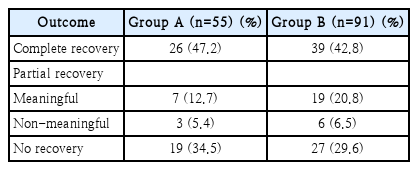
Hearing recovery after 1 month
ITS 시행 횟수에 따른 청력 호전 비교
A군에서 총 고실 내 스테로이드 주입술을 받은 횟수에 따라 4회 이하 시행한 군과 5회 이상 시행한 군으로 분류하였다.양 군의 청력 회복 정도를 2012 AAO-HNSF Clinical Practice Guidelines에 따라 분류하면, 4회 이상 시행한 군은 총 24명 중 완전회복을 보인 경우는 12명(50.0%), 유의미한 부분회복을 보인 경우는 1명(4.1%), 무의미한 부분회복을 보인 경우는 2명(8.3%)이었고, 회복이 없는 경우는 9명(37.5%)이었다. 5회 이상 시행한 군은 총 21명 중 완전회복을 보인 경우는 9명(29.0%), 유의미한 부분회복을 보인 경우는 7명(22.5%), 무의미한 부분회복을 보인 경우는 6명(19.3%)이었고, 회복이 없는 경우는 9명(29.0%)이었다. 완전회복군과 부분회복군을 청력 회복으로 간주하여 양 군 간의 회복률의 차이를 카이제곱 검정하였을 때, 유의미한 통계학적 차이는 없었다(p> 0.05)(Table 4).

Hearing recovery after 2 weeks (according to the number of intratympanic injection of steroid)
고실 내 스테로이드 주입술 시행 횟수에 따른 각각의 청력호전도를 선형회귀분석을 통해 비교하였을 때, 치료 2주 후(p=0.93)와 치료 1개월 후(p=0.38) 모두에서 고실 내 스테로이드 주입술 시행 횟수에 따른 청력 호전도의 유의미한 상관관계는 없었다(Fig. 3).

Hearing gain according to the number of ITS in the simultaneous SS with ITS group. There was no significant difference in hearing gain after 2 weeks (p>0.05) (A). There was no significant difference in hearing gain after 1 month of treatment (p>0.05) (B). SS: systemic steroid administration, ITS: intratympanic injection of steroid.
고 찰
본 연구는 경구 스테로이드와 고실 내 스테로이드 주입술을 동시에 병행한 군(A군)과 경구 스테로이드만 복용한 군(B군)의 청력 회복 정도를 2012 AAO-HNSF Clinical Practice Guideline에 따라 각각 치료 후 2주, 1개월 뒤 비교하였다. 치료 2주 후와 치료 1개월 후에서 A군과 B군 간에 청력역치 호전도는 유의미한 통계학적 차이는 없었다(p>0.05). 완전회복군과 부분회복군을 청력 회복으로 간주하여 두 군 간의 회복률의 차이를 비교하였을 때, 유의미한 통계학적 차이는 없었다(p>0.05).
전신 스테로이드 투약 및 고실 내 스테로이드 주입술을 병행한 치료 결과에 대해서 다양한 결과들이 보고되었다. Battalglia 등[9]은 경구 스테로이드 단독 투약한 군, 고실 내 스테로이드 주입술 단독 시행한 군, 두가지를 병행한 군의 치료 4주 후 청력 회복을 비교하였고, 병행치료한 군에서 나머지 두 군보다 회복률이 유의하게 높았다고 보고하였다. Jung 등[10]은 후향적 증례 대조군 연구로 전신 스테로이드만 투약한 군과 고실 내 스테로이드 주입술을 병행한 군을 비교하였다. 치료 후 10일 째에는 양 군 간에 유의한 차이는 없었으나, 90일 이후에는 병행치료 군에서 전 주파수에 걸쳐 더 높은 회복률을 보였다고 보고하였다. Gundogan 등[13]은 전향적 무작위 비교 연구로 경구 스테로이드 단독 투약한 군과 고실 내 스테로이드 주입술을 병행한 군을 비교하였다. 치료 시작 후 2주, 4주 째에 각각 청력 호전도를 Siegel’s criteria에 따라 비교하였고, 병행치료 군에서 전 주파수에 걸쳐 더 높은 회복률을 보였다고 보고하였다.
Ahn 등[14]은 전향적 연구로 경구 스테로이드 단독 투약한 군과 고실 내 스테로이드 주입술을 병행한 군을 비교하였다. 치료 시작 후 3개월째에 청력역치 호전도를 Siegel’s criteria에 따라 비교하였고, 두 군 간에 유의한 차이는 없었다. Ashtiani 등[15]은 경구 스테로이드 단독 투약한 군, 고실 내 스테로이드 주입술 단독 시행한 군, 그리고 두 가지를 같이 병행한 군으로 나누었고, 치료 시작 4주 후에 청력 회복률은 세 군 간에 유의미한 차이가 없었다고 보고하였다. Baysal 등[16]은 경구 스테로이드 단독 투약한 군과 고실 내 스테로이드 주입술을 병행한 군을 비교하였다. 치료 시작 후 1개월째에 청력역치 호전도는 두 군 간에 유의미한 차이가 없었다고 보고하였다.
이와 같이 전신 스테로이드와 고실 내 스테로이드 주입술 병행 치료 결과는 선행 연구에서 다양하게 보고되었다. 하지만 과거 연구들은 청력 호전도 비교 기준 또한 다양하였다. 반대 측 청력의 5 dB 이내, 병변 측 청력의 10 dB 이상 호전, Siegel’s criteria [18] 또는 연구자가 설정한 자체적인 기준을 적용하기도 하였다. 하지만 본 연구는 청력 회복 정도를 2012 AAO-HNSF Clinical Practice Guideline [17] 따라 분석하였고, 병행 치료와 단독 치료 사이에 청력 호전에는 유의한 차이가 없었음을 확인하였다.
A군에서 고실 내 스테로이드 주입술을 4회 이하로 시행한 군과 5회 이상 시행한 군을 비교하였을 때, 청력 회복의 유의미한 통계학적 차이는 없었다(p>0.05). 또한 고실 내 스테로이드 주입술 횟수에 따른 청력 회복에 유의한 차이는 없었다. 2012 AAO-HNSF Clinical Practice Guideline [17]에 따르면 고실 내 스테로이드 주입술은 초 치료 실패 시 또는 치료 후 불완전한 회복 시 시행하라고 권고되어 있다. 주입술의 횟수를 특별히 정의하지는 않았으며, 참고로 제시된 다양한 연구에서는 3회 또는 4회 고실 내 스테로이드 주입술을 시행하였다. 본 연구는 고실 내 스테로이드 주입술을 경구 스테로이드와 동시에 초기 치료로 시행했을 때의 효과를 확인하고자 하였으나 유의한 청력 호전 결과는 없었다. 따라서 고실 내 스테로이드 주입술은 초기 병행치료보다는 구제 치료로 시행되어야 하겠다.
본 연구는 후향적 의무기록 분석이기 때문에 두 군이 무작위 배정되지 않았다는 한계점이 있다. A군의 치료 전 초기 순음청력역치가 B군에 비해 유의하게 높았으며, 이는 치료 전 초기 청력 저하가 심했을 경우 고실 내 스테로이드 주입술 병행이 더 많았음을 시사한다. 이러한 한계점을 보완하고자 청력 저하 정도에 따라 2012 AAO-HNSF Clinical Practice Guideline(class A, PTA <30 dB and SDS >70%; class B, PTA >30 dB and <50 dB and SDS >50%; class C, PTA >50 dB and SDS >50%; Class D PTA any level and SDS <50%)와 같이 청력 저하 정도를 분류하여 추가 분석을 시행했다[19]. 각 군의 class별로 치료 한 달 후의 청력 회복 정도를 카이 제곱 분석했을 때, 모든 class에서 유의미한 차이는 나타나지 않았다. 본 연구는 치료 시작 후 1개월까지의 단기간 추적 관찰 결과만 비교하였으며, 치료 후 3개월 이상까지의 장기적 결과는 비교하지 못했다. 본 연구에서는 구제치료의 효과까지 고려하지 않았기 때문에 추후 고실 내 주입술 동시 치료 또는 경구 스테로이드 단독 치료 후 회복이 되지 않은 환자들에게는 추가적인 고실 내 스테로이드 구제 치료가 필요하겠다. 결론적으로 본 연구에서 경구 스테로이드제와 고실 내 스테로이드 주입술을 병행하여 시행한 군과 경구 스테로이드제만 투약한 군 간에 청력 호전도에 유의미한 차이가 없었으며, 더 많은 증례와 장기 추적 기간을 포함한 추가 연구가 필요할 것으로 보인다.
Acknowledgements
This work was supported by a National Research Foundation (NRF) of Korea grant funded by the Korean government (MSIT) (2020R1C1C1005965).
Notes
Author Contribution
Conceptualization: Eun-Ju Jeon, Hyun Jin Lee. Data curation: Kyungil Jang, So Yun Lim, Hyun Jin Lee. Formal analysis: So Yun Lim, Eun-Ju Jeon, Hyun Jin Lee. Funding acquisition: Hyun Jin Lee. Investigation: Hyun Jin Lee. Methodology: Eun-Ju Jeon. Project administration: Hyun Jin Lee. Supervision: Eun-Ju Jeon. Validation: Hyun Jin Lee. Visualization: Hyun Jin Lee. Writing—original draft: Kyungil Jang, Hyun Jin Lee. Writing—review & editing: Hyun Jin Lee.