상악동에 발생한 일차성 두개 외 수막종 1예
A Case of Primary Extracranial Meningioma in the Maxillary Sinus
Article information

Trans Abstract
Meningioma is one of the most common tumors of the central nervous system. However, primary extra cranial meningioma is rare as it consists 1%-2% of meningioma. It is very rare in paranasal sinus and accounts for about 0.1% of the paranasal sinus tumor. The treatment of choice is complete surgical excision of the tumor. Herein, with a review of the literature, we report a rare case of primary extra cranial meningioma in a 38-year-old male.
서 론
수막종은 중추신경계에서 기원하는 종양 중 가장 흔한 종양으로 두개 내 종양의 15%-20%를 차지하고, 두개 내에서의 연간 발생률은 100000명당 약 6명으로 알려져 있다[1]. 하지만 두개 외 영역에서는 잘 발생하지 않는 것으로 알려져 있고, 두개 외 영역에서 원발하는 경우는 전체 수막종의 약 1%-2% 정도를 차지한다. 두개 외 수막종은 안와에 가장 많이 발생하는 것으로 보고되고 있고, 그 이외에 귀, 코, 부비동, 이하선, 목, 인두 등에도 발생할 수 있다[2]. 부비동에 발생하는 두개 외 수막종은 매우 드문 질환으로, 부비동에 발생하는 종양의 약 0.1% 정도로 알려져 있다[3]. 국내에서는 사골동에서 원발한 수막종에 대한 증례가 1회 보고된 바 있지만, 상악동에서 원발한 수막종에 대한 증례는 보고된 바 없기에, 본 저자들은 상악동에 발생한 수막종 1예를 문헌 고찰과 함께 보고하는 바이다.
증 례
38세 남자 환자가 약 2개월 전부터 간헐적으로 발생하는 코막힘을 주소로, 타병원에서 촬영한 부비동 전산화 단층촬영(CT)과 조직검사에서 신경 섬유종이 의심되어 추가 검사 및 수술을 위해 본원으로 내원하였다. 내원 당시 코막힘 이외 콧물, 기침, 코피 등의 다른 증상은 호소하지 않았고 특이한과거 병력 및 수술 병력도 없었다. 외래에서 시행한 내시경 검사에서 조직검사 후 발생한 것으로 의심되는 유착 소견 외 다른 소견은 관찰되지 않았다(Fig. 1). 본원에서 촬영한 CT 소견에서 우측 상악동에 다수의 작은 석회화가 동반되는 종양이 확인되었으며, 영상의학과에서는 섬유조직이 풍부한 골화섬유종 혹은 신경섬유종으로 판독하였다(Fig. 2A and B). CT에서 두개골 윤곽이 종양의 침범 소견없이 잘 유지되어 있고, 종양이 두개 내 영역을 침범한 소견은 보이지 않아 두개외 영역에서 기원한 것으로 생각할 수 있었다(Fig. 2C). 부비동 자기공명영상(MRI)에서 우측 상악동을 가득 채우는 종양이 확인되었고, T1, T2 강조영상에서 저강도 신호를 보이며 균일한 조영 증강을 보였다(Fig. 3). 또한 종양에 분포하는 영양 동맥(nutrient artery)이 있는 것으로 판단되어 혈관조영술을 시행하였고, 병변으로 침입한 나비입천장동맥(sphenopalatine artery)에서 기원하는 영양 동맥이 발견되어 polyvinyl alcohol을 이용하여 색전술을 시행하였다(Fig. 4). 색전술 시행 2일 뒤 전신마취하에 내시경하 절제술(endoscopic sinus surgery)과 상악동 근치술(Caldwell-Luc operation)을 시행하여 수술을 진행하였다. 종물은 경계가 명확하였으나 단단하고 크기가 커서 내시경하 절제술만으로는 종물을 완전히 제거하는 데 한계가 있어 내시경하 절제술 및 상악동 근치술을 함께 시행하여 부분적으로 종물을 제거하면서 완전 절제를 시행하였다(Fig. 5). 병리조직학적 소견상 종양은 방추형의 세포(spindle cell)로 구성되어 있고 석회화를 동반하고 있었다. 종양 세포 핵의 비정형 소견(atypism)이나 유사분열(mitotic figure), 국소 괴사 소견은 관찰되지 않았다(Fig. 6A and B). 면역조직화학염색에서 pan-Cytokeratin 항체에 대해 음성을 보여 전이성 종양을 배제할 수 있었고, MIB-1 labelling index (LI)는 전체 종양 세포의 1% 미만에서 양성을 보여 1등급 수막종에 해당하는 섬유성 수막종으로 최종 진단되었다(Fig. 6C). 환자는 술후 7일째 퇴원하였으며 합병증 및 병변의 재발 소견없이 3개월간 외래 추적 관찰 중이다.

Pre-operation endoscopic imaging of right nasal cavity.
Preoperative CT scan. Paranasal sinus CT shows an expansile mass with multiple calcification in the right maxillary sinus on axial (A) and coronal view (B). C: Paranasal sinus CT shows well maintained bony contour of temporal bone skull base with foramen ovalis (arrow) on coronal view.

Magnetic resonance image of paranasal sinus shows expansile mass with low signal in T2 weighted image (A) T1 weighted image (B).
Right common carotid artery angiography, axial view. A: It shows tumor blush at the right maxillary sinus. Nutrient arterial supply is originated from the right sphenopalatine artery. B: The tumor disappeared after polyvinyl alcohol embolization through the sphenopalatine artery.
Gross image of meningioma. A: Intra-operative image of meningioma. B: Gross photo of meningioma after operation.

Pathological findings. A: The tumor cells admixed with dystrophic calcification form fascicles parallel or storiform pattern (H&E, ×100). B: The tumor consists of spindle cells without obvious mitotic figures or atypism (H&E, ×200). C: The MIB-1 (Ki-67) labelling index is less than 1% (MIB-1, ×400). H&E, hematoxylin and eosin.
고 찰
수막종은 대부분 두개 내 영역에서 발생하는 양성의 천천히 자라는 종양으로 알려져 있다. 두개 외 영역에서 원발하는 경우는 전체 수막종의 약 1%-2% 정도를 차지한다고 알려져 있으며 발생이 드물다. 비강에서는 주로 코, 상악동, 전두동에서 발생하며, 사골동에서도 발생할 수 있으나 접형동에서의 발생은 드물다. 두개 외 영역과 두개 내 영역의 해부학적 관계에 따라서 두개 외 수막종은 원발성, 이차성 종양으로 분류할 수 있다. 이차성 종양은 두개 내 영역으로부터 종양이 연결되어 있으며 대부분의 두개 외 수막종은 이차성 종양이다[4]. Daneshi 등[5]은 원발성 종양을 전이성 종양 혹은 이차성 종양과 정확하게 감별할 수 있도록 3가지 기준을 제시하였다(Table 1). 본 증례에서는 전산화단층촬영, 자기공명영상, 혈관조영술 등의 영상 검사뿐만 아니라, 수술을 통해서도 환자의 병변이 두개 내 연결이 없는 원발성 두개 외 수막종임을 확인할 수 있었다. 원발성 두개 외 수막종의 기원은 아직 정확히 밝혀지지 않았지만, 뇌신경의 말이집(myelin sheath)에 존재하는 지주막세포로부터 원발성 두개 외 수막종이 기원한다는 가설이 받아들여지고 있다[6]. 증상은 관련된 부비동에 따라 다양하게 나타날 수 있다. 전두동을 침범한 경우 안구돌출, 시력저하, 두통 등이 발생할 수 있고 상악동을 침범한 경우 뺨이 부을 수도 있다[7]. 영상학적으로 전산화단층촬영과 자기공명영상촬영이 수막종의 진단에 유용하다고 알려져 있다. T1 강조영상에서는 등강도 또는 약간의 저강도를 보일 수 있으며, T2 강조영상에서는 종양의 혈관분포상태나 석회화 정도에 따라 다양한 신호강도를 보일 수 있다. 수막종은 조직학적으로 수막세포형(meningotheliomatous), 섬유모세포형(fibroblastic), 이행형(transitional), 혈관종성(angiomatous), 미세낭형(microcystic) 등으로 분류할 수 있다. 최근에는 자기공명영상의 신호강도와 종양의 조직병리학적 아형의 연관성에 관한 연구 결과가 보고되고 있다. T1 강조영상은 수막종의 아형과 상관없이 비슷한 양상을 보이지만 섬유모세포성 수막종으로 확진된 경우 T2 강조영상에서 비교적 저강도 신호를 보인다고 알려져 있다[8]. 본 증례의 경우도 조직검사 후 다시 MRI 결과를 확인한 결과 섬유모세포성 수막종에 해당되는 소견을 확인할 수 있었다.

Three criteria to differentiate paranasal sinus meningiomas from metastatic meningioma or those extending from intracranial tumors
술전 정확한 수술 계획을 위해 전산화단층촬영, 자기공명영상 촬영 등이 필요하며, 영상에서 종양으로의 혈관 침범이 의심되면 혈관조영술 및 색전술을 시행하여 수술 중 발생할 수 있는 출혈의 위험성을 줄일 수 있다[9]. 본 증례의 경우에도 자기공명영상촬영 판독 중 영양 동맥이 확인되어 색전술을 시행한 후 수술을 진행하였다.
원발성 두개 외 수막종의 치료는 수술적 완전절제이다. 수막종은 방사선 저항성을 가지고 있는 종양이기 때문에 수술이 불가능하여 완화 치료를 고려하는 경우에서만 방사선 치료를 시행한다[10]. 병변이 충분히 제거된 경우 재발은 거의 없는 것으로 보고된다.
상악동에서 기원하고 국한된 원발성 두개 외 수막종은 국외에서 총 5예 보고되었고 국내에서는 보고된 바가 없었다. 국외에서 보고된 총 5예를 분석하였다(Table 2). 평균 연령은 26세였으며 남성이 4명(80%)으로 더 높은 비율을 차지하였다. Case 1, 4는 측비절개술로 수술을 시행하였으며[3,12], case 2는 구강 내 접근을 통해 첫 번째 어금니 및 송곳니와 함께 종괴를 절제하였다[8]. Case 3은 상악골전절체술로 종양을 전체 절제하였으며[11], case 5는 수술 방식이 묘사되어 있지 않았다[13].
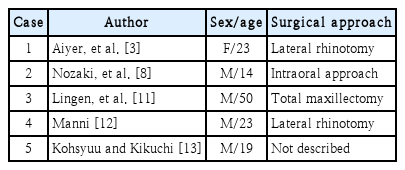
Summary of the characteristics of primary extra cranial meningioma from the maxillary sinus
대부분의 수막종은 원격 전이를 일으키지 않고 악성으로의 전환도 매우 드물기 때문에 정기적으로 추적 관찰하면 환자의 예후는 좋은 것으로 알려져 있다[3]. Ho 등[14]은 MIB-1 LI가 10% 미만인 수막종은 10년 이내 재발하지 않는다고 보고하였고, 병변의 충분한 절제와 낮은 MIB-1 LI가 수막종 경과의 좋은 예후 인자로 알려져 있다[15]. 본 증례에서는 MIB-1 LI가 전체 종양세포의 1% 미만으로 확인되었고 병변의 충분한 수술적 절제가 이루어져 예후는 좋을 것으로 예상된다.
Acknowledgements
None.
Notes
Author Contribution
Conceptualization: Woo Yong Bae. Data curation: Min Gyoung Pak. Formal analysis: Sangjun Kim. Investigation: Sang Hoo Park. Project administration: Woo Yong Bae. Supervision: Sangjun Kim. Writing—original draft: Sang Hoo Park. Writing—review & editing: Woo Yong Bae.