비인강으로의 아데노이드 확장 정도에 따른 방사선학적 지표와 수술 전후 삶의 질 비교
Comparison of Radiographic Parameters and Perioperative Quality of Life According to the Degree of Adenoid Extension to Choana
Article information

Trans Abstract
Background and Objectives
The aims of this study were to clarify the impact of adenoidal extension toward the choana on the quality of life and to find differences in radiographic parameters between patients needing additional excision with a 90-degree tip and those who only require a 40-degree debrider tip.
Subjects and Method
Patients who underwent adenoidectomy with both 40-degree and 90-degree debrider tips were defined as the difficult-to-treat (DTT) group. Patients who underwent adenoidectomy using only a 40-degree debrider tip were defined as the control group. We measured the antroadenoidal distance, the adenoidal nasopharyngeal ratio (ANR), the length from the adenoid to hard palate, and reviewed the Korean Obstructive Sleep Apnea-18 (KOSA-18) scale scores.
Results
There was no difference in the quality of life due to OSA between the DTT and control groups, pre- and post-operatively. Correlation analysis between the antroadenoidal distance and the pre-operative KOSA-18 scale scores revealed a negative correlation. The antroadenoidal distance was shorter in the DTT group; however, a cut-off value could not be obtained. The ANR was a statistically discriminatory, but not effective, factor.
Conclusion
There was no difference in the KOSA-18 scale scores between the groups with the adenoidal extension toward the choana and the control. The ANR should be considered in the pre-operative radiographic evaluation but is not a diagnostic parameter for choanal extension. Further studies to find additional parameters are necessary.
서 론
아데노이드 및 편도 비대는 소아 폐쇄성수면무호흡증(obstructive sleep apnea, OSA)에 관여하는 것으로 알려져 있다. 발병률은 연령에 따라 다르지만 소아 OSA는 반복적인 상부 호흡기 감염, 주간 피로, 성장 문제, 침 흘림 등의 증상을 유발한다고 알려져 있다[1].
OSA가 있는 소아 환자는 외과적 치료를 위해 이비인후과 의사의 진료 및 평가를 받는 것이 좋다. 이전 연구들의 결과에 따르면, 아데노이드 및 편도 절제술이 첫 번째 접근법으로 고려되어야 한다. 한 연구에 따르면 아데노이드 및 편도 절제술 후 무호흡-저호흡(apnea-hypopnea index) 지수가 현저하게 감소하여 OSA가 있는 소아 환자의 치료 및 삶의 질 향상에 효과가 있음을 시사했다[1].
아데노이드 절제 기술은 시간이 지남에 따라 발전했다. 여기에는 큐렛 아데노이드 절제술, 전기 소작 아데노신들 절제술, 골드 레이저를 이용한 아데노이드 절제술, 파워 아데노이드 절제술(powered adenoidectomy, PA), 내시경 보조 아데노이드 절제술 등이 포함되며[2-5], 그중 PA는 비강으로의 확장이 있는 아데노이드 조직을 완전히 제거하는 데 널리 사용되어 왔다. 40도 절삭기(debrider) 팁은 아데노이드 조직을 제거하기 위해 PA에서 흔히 사용되나 아데노이드 조직이 후비공(choana)에 근접할수록 절삭기 끝이 아데노이드로 접근이 어려워 완전히 절제하기가 어렵다. 이때 완전한 절제를 위해 추가적으로 90도 팁을 사용하여 제거를 시도하며 수술의 난이도가 높아진다.
따라서 적절한 수술 전 준비를 위해 아데노이드에 대한 평가가 이루어져야 한다. 아데노이드 크기를 측정하는 가장 직접적인 방법은 비인두경을 사용하는 것이다. 그러나 비인두경은 코 혹은 입안으로 내시경을 넣어 관찰해야 하기 때문에 소아 환자에게 도전적이고 불편하며 임상에서 사용하기가 쉽지 않다. 대신 방사선 데이터를 사용하여 아데노이드 크기를 평가하는 방법이 덜 침습적이고 내시경으로 측정하였을 때와 유의미하게 비슷하여 널리 사용해왔으며[6], 여러 연구들에서 측면 방사선 사진(lateral radiograph)을 통한 아데노이드 크기 측정을 위한 두부계측 매개변수(cephalometric parameters)들의 랜드마크(landmark)들이 정해져 왔다[7]. 또한 이전 연구에서 두부 계측 매개변수와 내시경 비인두경 검사 데이터는 수술 중 미러(mirror)를 통한 검사 결과와 연관성이 높은 것으로 나타났으며[8], adenoidal nasopharyngeal ratio (ANR)는 아데노이드의 크기를 측정하는데 가장 유의미한 변수로 알려져 있다[9].
아데노이드를 최대한 전절제하는 것이 아데노이드 절제술의 목표이나 잔여 아데노이드 조직으로 및 증상의 지속으로 인한 재수술의 가능성도 존재한다. 한 후향적 연구에 따르면 비후된 아데노이드가 후비공(choana) 공간을 75% 이상 막은 경우 재수술과 통계적으로 유의미하게 관계 있는 여러 인자 중 하나라고 보고하였다[10]. 따라서 수술 전 아데노이드에 대해 정확히 평가하고 수술 난이도를 예측하여 아데노이드를 효과적으로 절제하는 것이 중요하다.
이번 연구 목적은 후비공으로의 아데노이드 확장이 수술 전후 삶의 질에 차이를 주는지 분석하고, 아데노이드의 효과적인 전절제를 위해 90도 팁으로 추가 절제가 필요한 그룹과 필요 없는 그룹에서의 방사선 매개변수 차이를 비교하여 수술 전 수술 난이도를 예측함에 있어 유의미한 방사선 매개변수를 추가적으로 찾고자 한다.
대상 및 방법
대 상
2015년 4월부터 2017년 11월까지 강동경희대학교 이비인후과 외래에서 문진, 신체 검진으로 수면장애 진단을 받고 한 명의 의사에게 powered intracapsular tonsillectomy and adenoidectomy (PITA) 혹은 PA 수술을 받은 15세 미만의 소아 환자를 후향적 의무기록 검토를 통해 대상으로 포함하였다. 40도 및 90도 절삭기 팁으로 아데노이드 절제술을 받은 환자를 치료하기 어려운 difficult to treat (DTT)군으로 정의하였고, 40도 절삭기 팁만 사용하여 아데노이드 절제술을 받은 환자를 대조군으로 정의하였다. 재수술을 받은 환자, 두개 안면 기형이 있는 환자, 환기관 삽입, 설소대성형술, 고주파를 이용한 하비갑개 성형술과 같은 보조 수술을 받은 환자는 제외하였다. 178명의 환자(DTT군 89명과 대조군 89명)의 방사선 영상을 비교하였다. 연령, 성별, 증상, 수술 전 한국 폐쇄성 수면무호흡-18 (KOSA-18) 척도 점수, 수술 후 6개월 KOSA18 척도 점수 및 알레르기 검사 결과를 의무기록을 통해서 검토했다.
이 연구는 강동경희대병원의 Institutional Review Board (IRB)의 승인을 받았다(IRB No. 2016-04-029).
수술 자세와 방법
수술 시 시야 확보를 위하여 rose 위로(rose position) 위치시키고 환자의 어깨 밑으로 부드러운 어깨받침을 적용하고 정확한 비교를 위해 경부 및 두부의 신전 각도는 15도로 모든 환자에게 동일하게 적용하였다. 각도는 관절가동범위(range of motion)를 계측하는 여러 방법 중 관절각도측정기(universal goniometer)를 이용하는 방법을 선택하여 신전각도를 측정하였다. 경부 신전을 하기 전에 관절각도측정기의 중심부를 좌측 외이도 입구에 위치시킨 뒤 근위부 팔(proximal arm)을 지면과 수평하게 조정하고 원위부 팔(distal arm)을 지면과 수직으로 놓아 콧구멍이 있는 위치와 만나게 하여 90도 각도를 이루도록 조정한다. 그 후 경부를 신전하였으며 원위부 팔(distal arm)의 끝에 위치한 콧구멍이 이동한 각도가 15도를 이루는지 확인하였다[11]. 아데노이드 절제술은 전신마취하 8 french nelaton 카테터를 양 비강에 각각 1개씩 통과시켜 연구개를 앞쪽으로 견인한 뒤 미러를 이용하여 아데노이드 조직을 확인하면서 절삭기로 조직을 제거하였다.
방사선 변수 계측 방법
몇 가지 방사선 매개변수가 정의되었다. 기존의 많은 연구들에서 두부계측 매개변수에서의 랜드마크가 되는 지점들이 정의되었고, 그중 이번 연구에서 중요하게 생각되는 지점을 선정하여 매개변수를 설정하였다. 먼저, 기저후두골(basiocciput) 전방 가장자리 직선 부분에 가상의 선을 그렸다. ‘Adenoidal space (A)’는 기저후두골 전방 가장자리 직선 부분에서 아데노이드의 전방 경계에서 가장 큰 굴곡을 갖는 지점까지의 거리를 지칭하며, 아데노이드 공간의 선형 측정값이다. ‘Nasopharyngeal space (NpS)’는 경구개판의 후상방 끝 지점과 접형후두연골결합부(spheno-occipital synchondrosis)의 전하방 경계까지의 거리로 정하였으며, 비인두 공간의 선형 측정값이다. ‘Antroadenoidal distance (AA)’는 후비공(choana)과 같은 선상에 놓여있는 상악동의 후방 벽부터 아데노이드의 전방 경계까지의 가장 짧은 거리로 하였다. ‘Adenoidhard palate distance (AH)’는 경구개판의 후상방 끝 지점부터 아데노이드의 전방 경계까지의 거리로 하였다. “ANR’은 아데노이드 공간과 비인두 공간의 비율을 뜻하며 아데노이드 공간의 선형 측정 값인 ‘A’와 비인두 공간의 선형 측정값인 ‘NpS’의 비율로 계산하였다[9]. 이러한 모든 데이터들은 한 명의 의사가 측정하였다(Fig. 1).

Indications in lateral radiograph. A, greatest distance between a line drawn along the straight part of the inferior margin of the basiocciput and the point of maximal convexity on the anterior outline of the adenoid; AA, antroadenoidal distance (shortest distance between the anterior outline of the adenoid and posterior wall of the maxillary antrum, which lies in the same plane as the posterior choana); AH, distance between the posterior and superior edge of the hard palate and the point on the anterior outline of the adenoid used to measure AA; NpS, distance between the posterior and superior edge of the hard palate and anteroinferior margin of the sphenobasioccipital synchondrosis.
수면설문작성
KOSA-18 설문지는 Franco 등[12]이 발표한 OSA-18 설문지를 한글로 번역한 것으로, 아동의 수면과 관련된 삶의 질을 평가할 수 있는 도구이다. KOSA-18 설문지는 아동의 삶의 질에 대해 18가지 질문으로 구성되어 있다. 각 항목들은 다음과 같은 5가지의 하위 그룹으로 나눌 수 있다. ‘수면상태’, ‘신체적 증상’, ‘정서적 증상’, ‘낮 시간의 생활’, ‘부모의 상태’, 각 항목에 대한 점수는 1점(전혀 없다)부터 7점(항상 그렇다)까지 이며 총점은 18점부터 126점까지의 범위를 가진다[13]. KOSA18의 총 점수에 따라서 삶의 질에 미치는 영향의 정도는 KOSA-18의 총점이 60점 미만인 경우는 삶의 질에 적은 영향(small impact), 60점 이상 80점 미만은 중간 영향(moderate impact), 80점 이상은 많은 영향(large impact)을 끼치는 것으로 하였다.
통계 분석
DTT군과 대조군(control group)은 Student’s t-test를 사용하여 비교분석 하였다. 수술 전 KOSA-18 점수와 수술 후 KOSA-18 점수는 paired t-test를 이용하여 분석하였다. 이 통계에서 기준치 값(cut-off value)은 receiver operating characteristics (ROC) curve를 통해 계산하였다. 통계적 유의미한 차이는 p<0.05일 때로 고려하였으며, 통계적 분석은 SPSS 20 package (IBM Corp., Armonk, NY, USA)를 사용하여 이루어졌다.
결 과
DTT군과 대조군의 평균 연령 및 성별 분포는 유의한 차이가 없었다. 두 그룹 모두 PITA를 받은 환자가 PA를 받은 환자보다 많았지만 두 그룹 간의 비율에는 차이가 없었다. 두 그룹 모두 수술 전후 KOSA-18 점수 사이에 유의한 차이가 없었다(Table 1).
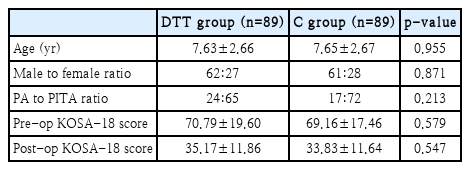
Demographic data of patients who underwent powered adenotonsillectomy or adenoidectomy
DTT군과 대조군은 수술 전후 KOSA-18 점수 분포에 큰 차이가 없었으며 두 그룹 간에 OSA로 인한 삶의 질에는 차이가 없었다(Table 2). 즉, 수술 전 두 그룹 간에 많은 영향력 끼친다고 답한 사례의 분포에 유의미한 차이가 없었으며, 수술 후 두 그룹 간의 적은 영향력을 끼친다고 답한 사례 분포에 유의한 차이 또한 없었다.

Comparison of the pre- and post-operative KOSA-18 scores
편도선의 비대가 수면무호흡 증상에 영향을 미칠 수 있고, 수술 후 증상 개선에 영향을 미친 변수가 될 수 있어 각 그룹 내에서 편도선절제술을 같이 시행한 환자를 제외하고 PA만 시행한 환자들의 KOSA-18 척도 점수를 비교했다. DTT군과 대조군은 수술 전후 그룹별 분포에서 유의한 차이를 보이지 않았다(Table 3).

Comparison of the pre-operative and post-operative KOSA-18 scores in patients who underwent powered adenoidectomy
AA와 수술 전 KOSA-18 척도 점수 간의 상관 관계 분석은 음의 상관관계를 나타냈다(Spearman의 rho=-0.174, p=0.026). 또한 ANR과 수술 전 KOSA-18 점수 사이에는 상관관계가 없었다.
AA는 DTT군에서 더 짧았다. 기준치 값은 DTT군에서 환자를 식별하기 위한 기준을 제공하기 위해 계산되었다(Table 4). 그러나 AA의 ROC 곡선에서 곡선 아래 면적이 0.5 미만이므로 기준치 값을 얻을 수 없었다. ANR의 ROC 곡선 아래 면적은 0.668로 변별력을 갖는 인자였으나, ANR 값이 최적 절단점(optimal cut point)인 0.62일 때 DTT군의 환자를 나타내는 민감도와 특이도는 각각 57.3%와 55.6%였다. 불행하게도 이것은 진단의 척도로 지정하기에 효율적인 기준치 값이 아니었다(Fig. 2).
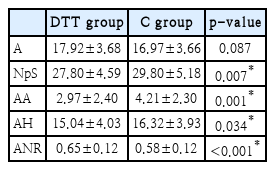
Comparison of radiographic parameters in the DTT group and C group
Receiver operating characteristic curve of AA and ANR. AA, antroadenoidal distance (shortest distance between the anterior outline of the adenoid and posterior wall of the maxillary antrum, which lies in the same plane as the posterior choana); ANR, adenoidal nasopharyngeal ratio (ratio between the adenoid and nasopharyngeal space); AUC, area under the curve.
고 찰
이번 연구에서 저자들은 후비공으로의 확장이 있는 아데노이드 비후 소아 환자에서 진단적 가치가 있는 방사선 매개변수에 대해 알아보고, 후비공 확장이 수술 전후 수면 질 개선에 차이를 주는지 평가하였다. 소아의 수면무호흡은 성인의 수면무호흡과 진단적 기준이 다르며 여러 연구의 메타 분석을 통해 소아 OSA의 전체 유병률은 7.45%로 보고되었다[14]. 소아 OSA는 빠른 안구 운동 수면(rapid eye movement [REM] sleep)의 발생을 증가시켜 이산화탄소 저류를 유도하고 상악, 하악 발달에 영향을 준다. 야간 수면 검사실에서 시행하는 수면다원검사는 소아 OSA의 진단 및 평가를 위한 일차적인 기준(gold standard)으로 간주된다. 그러나 아이들은 협조가 잘되지 않아 수면다원검사를 받기가 어려우며, 대안으로 몇가지 설문지가 개발되어 높은 민감도와 특이도로 진단에 사용되고 있다. 그중 KOSA-18은 한국에서 널리 사용되고 있다[15].
방사선 사진은 후비공에서 아데노이드가 차지하는 단면적을 결정하기 어렵지만 측면의 매개변수 데이터를 제공할 수 있다는 장점이 있다. 증상과의 상관 관계를 보여주는 방사선 매개변수를 찾기 위한 연구가 수행되었으며, 이전의 한 연구에 따르면 AA가 작을수록 구호흡과 코골이를 반영하는 증상 점수가 높아진다고 보고하였다[16]. 본 연구에서는 AA와 KOSA-18 사이에 음의 상관 관계가 확인되었으나 방사선학적 수치는 비디오 비내시경(rhinoscopy)에 의해 추정된 수치보다 증상의 정도와 더 낮은 상관 관계를 보였으며[15], 후비공으로 확장의 변별력을 갖는 기준값이 되지는 못했다.
잔여 아데노이드 조직은 코골이, 코 막힘, 세균의 저장창고 기능, 남아있는 조직의 증식과 같은 문제를 일으킬 수 있으므로 대부분의 아데노이드 조직을 절제하는 것이 중요하다. 아데노이드 조직을 가능한 한 많이 제거하기 위해 소파술, 흡인 투열성 절제, 고주파 절제, 아데노이드 펀치 겸자 및 PA를 포함한 여러 방법이 제안되었고[17], 이번 연구에서는 PA를 시행한 환자를 대상으로 분석을 시행하였다.
DTT군 및 대조군에서 수술 전 KOSA-18 척도 점수 분포를 비교하면 choanal adenoid 조직은 수면무호흡증으로 인한 삶의 질에 기여하지 않을 수 있다. 또한 DTT군과 대조군에서 수술 후 KOSA-18 척도 점수의 분포도 다르지 않았다. 편도선 비대로 인한 효과를 제거하기 위해 동일한 조건에서 PA를 받은 환자를 비교했으며, 이 때에도 DTT와 대조군 사이에는 큰 차이가 없었다.
방사선 데이터를 통한 비교에서 DTT군과 대조군 사이의 NpS, AA, ANR 및 AH의 유의한 차이가 발견되었다. 해부학적으로 보았을 때 후비공으로 확장된 아데노이드의 크기와 밀접하게 관련된 매개변수가 ‘AA’이기 때문에 ‘AA’를 사용하여 DTT군에서 환자를 식별하기 위한 컷오프 값을 제시하려고 시도하였지만 AA의 ROC curve 밑 면적이 0.5 미만으로 식별력이 낮아 ANR을 이용하여 기준치 값을 얻었다. 그러나 ANR이 0.62 이상인 경우 DTT군 환자 식별 민감도는 57.3%로 높지 않았기 때문에 ANR은 DTT 그룹에 속하는 환자를 예측하는 데 유용한 기준이 아니라고 볼 수 있었다.
이 연구는 수술 전 아데노이드의 후비공 확장이 있는 경우에는 완전한 전제를 위해 고전적으로 크기 측정 변수로 사용되었던 ANR값 외에 고려해야 할 다른 방사선 매개변수가 필요함을 제시하고 있다. 민감도와 특이도가 높은 다른 매개변수를 찾기 위해 추가 연구를 수행해야 할 필요가 있다.
결론적으로, 후비공으로 아데노이드 확장에 있어 90도 절삭기 팁이 추가적으로 필요한 군과 필요하지 않은 군에서 KOSA-18 점수는 차이가 없었다. 후비공으로 아데노이드 확장이 있는 환자는 더 짧은 비인두 공간, 더 짧은 AA, 더 짧은 아데노이드-경구개 거리 및 더 큰 ANR을 갖지만, 수술 전 수술 난이도를 평가함에 있어 유의미한 변수는 아니었다. 따라서 민감도와 특이도가 높은 다른 매개변수를 찾기 위해 추가 연구를 수행해야 할 필요가 있다.
Acknowledgements
None
Notes
Author Contribution
Conceptualization: Kun Hee Lee. Data curation: Seok Hyun Kim. Formal analysis: Jong Hwan Lee. Investigation: Seung Yup Son. Methodology: Kun Hee Lee. Project administration: Je Ho Bang, Seok Hyun Kim. Writing—original draft: Je Ho Bang. Writing—review & editing: Je Ho Bang, Kun Hee Lee.