효과적인 BAHAⓇ Attract의 이식술식
A Novel Surgical Technique for BAHA® Attract Implantation
Article information

Trans Abstract
An implantable bone conduction hearing aid is a device that assists hearing by transmitting sound vibration through the bone. It is suitable not only for patients with conductive hearing loss and congenital external aural atresia but also for those with unilateral hearing loss, chronic otitis media, or patients whose normal structure has been destroyed due to previous surgery. In this paper, we introduce a novel surgical technique for an implantable bone conduction hearing aid (BAHA® Attract) that can be performed through minimal incision in a short time under local anesthesia based on accurate anatomical characteristics. We believe this novel technique could provide convenience for patients and surgeons. Additionally, through this technique, we can expect that various types of implantable bone conduction hearing aids that function effectively and safely can be provided for patients.
서 론
골전도 보청기(bone conduction hearing aid)는 골도 청력을 활용하여 소리를 듣게 하는 청각 보조기기이다. 소리 자극은 내이의 달팽이관에서 전기 신호 형태로 변환된 후 청신경을 따라 청각 피질에 전달되고, 이 신호들은 뇌에서 소리로 전환되어 소리를 인지하게 된다. 이때 소리 자극이 달팽이관으로 도달하는 경로는 기도 경로와 골도 경로 두 가지이다. 기도 경로는 외이도를 통해서 들어온 공기의 진동이 고막과 이소골을 물리적으로 자극함으로써 이소골과 연결된 달팽이관으로 전달되는 경로를 뜻한다. 골도 경로는 두개골이나 연골, 피부, 연부 조직 등을 통하여 측두골 내에 존재하는 달팽이관에 진동을 전달함으로써 에너지가 전달되는 경로를 뜻한다. 골전도 보청기는 이런 골도 청력을 이용한 청력 보조기기로 고전적인 보청기와는 달리 외이도가 아닌 측두골 등에 수신기를 위치시켜 진동을 측두골 내 달팽이관에 전달한다. 그중에서도 이식형 골전도 보청기(bone conduction implant)는 외과적 수술을 통해 두개골에 기계를 이식하여 소리를 전달하는 보조기기를 뜻한다.
이식형 골전도 보청기는 크게 두 가지 형식으로 나눌 수 있다. 첫째는 피부 구동 방식(skin drive)으로, 소리 신호는 외부 장치에서 기계적 진동으로 변환된 뒤 피부를 경유하여(passive transcutaneous) 두개골 내에 이식되어 있는 내부 기기로 전달된다. 대표적으로 BAHAⓇ Attract (CochlearTM, Sydney, Australia)가 있다. 둘째는 직접 구동 방식(direct drive)이며 이는 다시 경피 접합(percutaneous) 방식과 능동 피하(active transcutaneous) 방식으로 나눌 수 있다. 경피 접합 방식은 BAHA (CochlearTM)를 대표로 하는 방식으로, 외부 장치는 소리 신호를 진동으로 변환시킨 뒤 두개골에 이식된 screw를 통해 이를 두개골로 전달한다. 외부 장치와 두개골을 연결하기 위해 불가피하게 피부에 육안으로 확인되는 screw를 이식하게 됨으로써 피부 괴사 및 감염 등의 우려가 있고 미용적으로 만족도가 떨어진다. 능동 피하 방식은 BonebridgeⓇ (MED-EL, Innsbruk, Austria), Osia2Ⓡ (CochlearTM)을 대표로 하는 방식으로, 앞서 소개한 피부 구동 방식과는 달리 외부 장치는 피부를 경유하여 두개골 내에 이식된 내부 기기로 소리를 전달해 주고, 내부 기기가 이 소리를 받아 진동으로 변환시켜 달팽이관으로 전달한다. 진동 에너지가 두개골 내에서 직접 발생하기에 에너지 소실이 적다는 장점이 있지만 내부 기기가 다른 방식의 내부 기기에 비해 크기 때문에 수술 시 위치 선정 및 술식이 좀 더 어려워진다는 단점이 있다. 이 세 가지 방식의 이식형 골전도 보청기는 환자의 나이, 수술력, 청력 및 술자의 경험과 선호도 등을 고려하여 선택해야 할 것이며, 현재까지 이들의 청력 개선 정도는 비슷한 것으로 알려져 있다[1]. 그러나 국내에서는 이식형 골전도 보청기가 많이 보급되지 못하고 있다. 이는 아마도 기계 이식에 대한 거부감, 수술에 대한 우려나 부작용에 대한 걱정 및 비교적 고가의 기계 및 수술 비용 등이 원인일 것으로 생각된다. 또한 비록 이식형 골전도 보청기의 기술이 계속 발전하고 있지만 아직까지 완벽한 품질의 소리를 제공하는 것은 아니며, 확실한 효과를 보이는 적응증도 상당히 제한적이다.
이식형 골전도 보청기는 전음성, 혼합성 난청 환자 및 일측성 난청 환자에게 적용할 수 있다. 특히 만성 중이염 등으로 소리를 전달하는 이소골이 소실되었거나, 이관의 만성적인 기능 저하로 효과적인 이소골 재건이 불가능한 경우에 훌륭한 치료 옵션이 될 수 있다. 그러나 한편으로는 이러한 이유 때문에 술자들이 수술 결정을 주저하게 되어 수술 경험이 적어지고, 적응증의 확장이 되지 못하는 악순환을 겪게 되기도 한다. 이를 해결하고자 저자들은 다음과 같은 노력을 하고 있다. 1) 최소 침습적인 수술 방법 개발: 기존 수술 기술을 개선하여 작은 절개선과 적은 노출 면적을 허용하는 최소 침습적인 수술 방법을 개발하고자 한다. 이를 통해 수술 후의 통증, 합병증 및 회복 기간을 줄일 수 있을 것이다. 2) 새로운 적응증 발견: 연구 및 임상 실습을 통해 이식형 골전도 보청기의 이점을 알리고 적응증을 확장시킬 수 있다. 기존의 양측성 선천성 이 기형 환자뿐 아니라 예를 들어 일측성 난청이나 중이염 수술을 대체하고자 하는 목적으로도 이식형 골전도 보청기를 적용할 수 있을 것이다[2,3]. 3) 근거에 기반한 수술 경험 마련: 인공와우 등 다른 임플란트 수술과는 다른 수술에 대한 근거를 마련하고, 충분한 연구와 임상 경험을 통해 이식형 골전도 보청기의 효과와 안전성을 입증할 수 있다. 이를 통해 술자들은 더 자신감을 가지고 수술을 시행할 수 있게 될 것이다. 4) 교육 및 정보 공유: 기업과 전문가들과 협력하여 이식형 골전도 보청기 커뮤니티를 만들고, 시뮬레이션 센터를 만들어 술자들에게 이식형 골전도 보청기에 대한 교육과 정보를 제공할 수 있을 것이다[4-6]. 이를 통해 의사들은 해당 기술에 대한 이해도를 높이고, 환자들에게 적합한 치료 옵션을 자신있게 제시할 수 있다.
이식형 골전도 보청기가 위치하는 측두골에는 S자 정맥동(sigmoid sinus), 근육, 신경 등 다양한 중요한 구조물들이 존재하고 있다. 이를 피하여 내부 기기가 위치하는 편평한 공간을 확보해야 하며, 과거 수술력으로 인하여 구조물이 많이 손상된 경우에는 내부 기기를 안전하게 이식하는 것이 쉽지 않고 또 미용적인 부분에서도 불만족스러울 수 있다. 이에 저자들은 정확한 해부학적 특성에 근거하여 부분 마취하에 짧은 시간 내에 시행할 수 있는, ‘수술’이 아닌 ‘시술’의 개념으로 진행할 수 있는 BAHAⓇ Attract의 이식술식을 소개하고자 한다.
방 법
본 연구는 의학 연구 윤리 심의 위원회(IRB No. 2016-11-0006)의 심의 및 승인하에 시행되었다.
이식 부위 선정
본 연구자들은 안전하고 효과적인 이식 부위로 다음과 같은 조건을 충족하는 부위를 찾고자 했다. 내부 기기는 제조사에서 제시한 바와 같이 외이도로부터 50-70 mm 거리에 위치하게 되며, 이에 맞춰 외부 장치를 착용했을 때 장치의 상단이 귓바퀴의 상단과 동일하게 위치하여야 한다. Screw의 안전한 접합을 위하여 최소 4 mm 이상의 골 두께가 보장되어야 하며, 효과적인 진동 전달을 위해서 이식 부위의 두개골은 굴곡이 없도록 드릴 작업 등을 통해 약 지름 27 mm 원형의 implant magnet이 최대한 많이 접촉되도록 해야 한다. Sigmoid sinus 등 주위의 위험한 구조물에 내부 기기가 접합되지 않도록 하여야 하며, 가급적 절개선을 피하여 외부 장치와 내부 기기가 부착될 수 있도록 하여야 한다. 마지막으로 미용적인 면을 고려하여 절개선의 크기나 위치가 가능한 작고 눈에 띄지 않는 부위를 선택할 수 있다면 환자의 만족도를 더 증진시킬 수 있을 것이다.
본 연구자들은 총 20구의 카데바를 이용해 총 40개의 측두골을 관찰하였고, 위 조건을 충족하는 위치를 선정하였다[7-9]. 이 위치는 다음의 경계로 이루어져 있다. 전방 경계는 sigmoid sinus, 후방 경계는 occipitomastoid suture line, 상방 경계는 asterion으로부터 temporal line을 연결한 선이며 하방 경계는 digastric groove의 상방 경계를 temporal line과 평행하게 연결한 선이다(Fig. 1A). 제조사에서 권유했던 부위가 비교적 기존의 이과 수술의 접근법으로 쉽게 접근할 수 있는 대신 두개골의 suture line 등으로 인해 드릴 작업이 필요했던 것에 비하면 이 구역은 측두골 중 비교적 평평하고 넓으며 충분한 골 두께가 보장되어, 추가적인 드릴 작업 없이도 지름 3 cm 가량의 implant magnet을 충분하게 접촉시킬수 있고, 비교적 안전하게 implant screw를 이식할 수 있다는 장점이 있다(Fig. 1B). 또한 상기 경계가 되는 해부학적 구조물은 좌, 우와 관계없이 40개의 측두골에서 구조물 사이의 거리에 유의한 차이를 보이지 않았으며, 기존의 이과 수술력과 무관하게 landmark로 사용할 수 있다는 장점이 있다(Fig. 2).

Suggested optimal position for the BAHA® Attract (CochlearTM) implant. A: The four borders of the optimal surgical site (OSS); anterior: sigmoid sinus line (SL), posterior: occipitomastoid suture line (OMS), superior: asterion line (AL) which connects the temporal line from the asterion, and inferior: digastric groove line (DL) which connects the upper boundary of the digastric groove parallel to the temporal line. B: The anatomical distribution of the temporal bone shows that the OSS, with a relatively flat surface, is a better position for the BAHA® Attract implant. CSS, conventional surgical site.
Comparison of the distance between structures within the temporal bone. There was no difference between the right and left sides. A: The distance from the spine of Henle (HS) to the sigmoid sinus. Right: 2.04±0.01 cm, Left: 2.14±0.10 cm (p=0.499). B: The distance from the HS to the asterion. Right: 5.05±0.09 cm, left: 4.97±0.07 cm (p=0.479). C: The area of the optimal surgical site. Right: 3.74±0.24 cm2, left: 3.37±0.18 cm2 (p=0.225). SS, sigmoid sinus.
이식술식
이와 같은 연구 결과를 토대로 본 연구진은 최소 절개선을 이용하여 BAHAⓇ Attract를 이식할 수 있는 다음 술식을 고안하였다. 상방 경계인 temporal line 및 하방 경계인 digastric groove의 상단에서 temporal line과 평행한 선을 그어 이식 부위의 상하 경계를 설정한다. 이후 귀 이개 후면을 촉지하여 Henle’s spine을 찾은 뒤, 상방 경계 즉 temporal line과 약 4 cm 거리에서 만나는 지점인 asterion과, 약 2 cm 거리의 구조물인 sigmoid sinus를 표시한다. 이 사이에 엄지바닥을 대고, 평편한 위치를 촉진해 본다. 이를 통해 상술한 최적의 이식 위치를 설정할 수 있다. Implant magnet은 엄지 손가락 첫째 마디 바닥의 크기와 비슷한 27 mm의 지름을 가진 원의 형태로, 상단이 귓바퀴의 상단보다 높게 위치하지 않도록 하고, hair line보다 1-2 mm 이상 후방으로 위치하도록 하여 추후 절개선이 될 hair line과 겹치지 않도록 한다. 확정된 이식 위치를 토대로, hair line을 따라 약 2.5 cm의 절개선을 가한다. 이후 견인기를 이용하여 시야를 확보하고 periosteum에는 screw의 위치에 맞게 십자 incision을 넣어 조직 손상을 최소화하도록 한다. 이후 제조사의 protocol에 따라 내부 기기를 모두 이식한 뒤 skin suture 후 마무리한다. 이때 bone polishing을 위한 drilling은 필요하지 않다(Fig. 3, Supplementary Video 1).

Schematic drawing of the newly developed surgical procedure for implantation of BAHA® Attract (CochlearTM). A: The small incision line along the patient’s hairline was marked. B: The soft tissue thickness was measured with a thin needle. C: An incision was made down to the periosteum. D: The implant magnet template was placed on the periosteum. E: A cruciate incision was made on the periosteum, and the periosteum was lifted. F: The bone was drilled with a guide drill to a depth of 4 mm. G: The hole was widened with the widening drill. H: The implant was placed with a torque of 40–50 N-cm. I: The bone bed indicator was used to confirm that the implant did not touch the bone or periosteum around the implant. J: The thickness of the flap was evaluated with the soft tissue gauge, and should be 3–6 mm. If the skin flap was thicker than the reference point, the flap was thinned to 6 mm. K: The implanted magnet was attached and screwed clockwise. L: The skin was sutured to the periosteum over the implanted magnet. The guide drill, widening drill, torque, bone bed indicator, soft tissue gauge, and screw driver are included in BAHA® Attract system.
증례 보고
본 연구자들은 3인의 환자에게 상기 술식을 이용하여 BAHAⓇ Attract를 이식하였다[7]. 각 환자의 정보는 다음과 같다(Table 1). 본 연구진은 혼합성 난청과 일측성 난청에서 BAHAⓇ Attract를 나누어 시행하였으며, 혼합성 난청의 경우 고식적인 만성 중이염 수술 이후에도 청력개선 효과가 없는 환자를, 일측성 난청의 경우 돌발성 난청 환자를 대상으로 하였다. 수술은 전신 마취가 아닌 부분 마취로 시행되었으며, 절개선의 크기는 평균 25 mm였고 수술 시간은 평균 22분 정도 소요되었다[7]. 수술 직후 어지럼증, 통증 또는 수술 부위 관련된 합병증은 없었으며, 술후 10일 뒤 실밥을 제거하고 1달 뒤 외부 장치를 착용하였다. 절개선은 hair line을 따라 시행되었기에 눈에 잘 띄지 않았고, 모발이 자라지 않는다거나 모자나 안경을 쓸 때 외부 장치와 간섭이 생기는 일은 발생하지 않았다(Fig. 4). 외부 장치 착용 후 2개월째와 6개월째 각각 시행한 청력 검사 및 소음하 청취 능력 평가에서도 만족할 만한 청력 증진을 확인하였다(Fig. 5). 또한 설문지에 의한 청력 개선에 대한 만족감의 향상 역시 확인할 수 있었다.
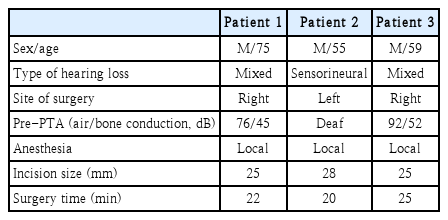
Patients’ characteristics

Postoperative findings of the surgical site. A: At postoperative 2 weeks (arrowheads: incision line). B: At postoperative 2 months.
Pre- and post-operative audiologic results. Average functional hearing gain was approximately 40 dB in all three patients. Hearing in Noise Test shows rapid improvement at initial, and gradual improvement during the 6-months follow-up. PTA, pure-tone audiometry; HINT, hearing in noise test.
고 찰
본 연구에서는 CochlearTM 사의 BAHAⓇ Attract의 효과적인 이식술식에 대해 소개하였다. 본 연구진은 추가적인 드릴 작업 없이도 지름 3 cm 가량의 implant magnet을 충분하게 접촉시킬 수 있는 공간을 찾을 수 있다면, 절개선의 크기나 노출 면적이 비교적 적어질 수 있다는 점에 착안하여 이상적인 이식 위치를 찾고자 노력하였다. 이에 40개 측두골의 해부학적 구조를 연구한 결과, 성별이나 방향에 관계없이 주요 구조물의 거리는 비교적 일정하다는 사실을 확인하였고, 이를 토대로 최소한의 절개선 및 최소한의 조작만으로 이식을 시행할 수 있는 술식을 고안하였다.
제조사에서 제공한 guide에 따른 C-shape 절개선은 두개골 노출이 용이하여 수술 중 시야 확보는 물론, 쉽게 추가 조작을 할 수 있지만 불가피하게 절개 범위가 커질 수밖에 없다. 본 연구에서 선정한 이식 부위는 두개골 내 드릴 작업이 필요하지 않기 때문에 두개골의 노출 부위를 최소화할 수 있어 절개선이 작아지며, 노출 부위 및 수술 부위 조작이 적어지면서 수술시간이 단축된다. 절개선이 작아짐으로써 수술 시간을 단축시킴은 물론 술후 회복 과정 및 후유증 등에서 좀더 자유로울 수 있었으며, 환자의 만족도 역시 높일 수 있다. 특히 hair line에 맞추어 절개선을 디자인함으로써 절개선의 흉터가 눈에 띄거나, 혹은 절개 부위의 모발이 새로 자라지 않는 부작용을 피할 수 있었다. 또한 이식 부위 역시 제조사에서 제공한 guide에 따른 부위보다 더 후하방에 위치함으로써 모자나 안경을 쓸 때 외부 장치와 간섭이 발생하는 일을 방지할 수 있었다.
본 연구에서는 해부학적 연구를 바탕으로 BAHAⓇ Attract의 안전하고 효과적이며 미용적으로 우수한 이식 술식을 소개하였다. 본 술식을 통해 향후 다양한 환자에게서 이식형 골전도 보청기는 물론 다양한 이식형 청각 기기의 적용 시 비 침습적이면서도 기능적으로 우수한 술식을 제공하는 좋은 근거가 될 수 있을 것으로 기대된다.
Supplementary Material
The Data Supplement is available with this article at https://doi.org/10.3342/kjorl-hns.2023.00759.
Acknowledgements
This research was supported by “Regional Innovation Strategy (RIS)” through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (MOE) to YJS (2022RIS-005). This research was also supported by the NRF grants funded by the Korea government (MSIT) to JML (2022R1F1A1071824).
Notes
Author Contribution
Conceptualization: Jeon Mi Lee, Young Joon Seo. Data curation: Young Joon Seo. Formal analysis: Young Joon Seo. Funding acquisition: Jeon Mi Lee, Young Joon Seo. Investigation: Young Joon Seo. Writing—original draft: Jeon Mi Lee. Writing—review & editing: Jeon Mi Lee, Young Joon Seo.