연령에 따른 이명 특성의 변화
Age-Related Variations in Tinnitus Characteristics
Article information

Trans Abstract
Background and Objectives
Tinnitus research faces challenges due to the variability of patient profiles. This study examines age-related differences in the characteristics and associated factors of tinnitus in a large patient cohort.
Subjects and Method
From January 2019 to March 2021, 439 tinnitus patients (596 affected ears) were assessed. Evaluations included pure tone audiometry, psychoacoustic testing, the Tinnitus Handicap Inventory (THI), and Visual Analog Scale (VAS) scores. Surveys also captured data on initial noise exposure, stress, fatigue, emotional shock, and accident/injury at tinnitus onset. We also assessed comorbidities such as hyperacusis, headaches, dizziness, neck/jaw pain, and psychiatric symptoms. Patients were grouped into young (≤30 years), middle-aged (31-49 years), and elderly (≥50 years) categories.
Results
Although tinnitus severity indicated by VAS annoyance and THI scores did not vary significantly with age, matched loudness (dB SL) was notably higher in the young and middle-aged groups compared to the elderly. Additionally, tinnitus awareness time was significantly longer in the elderly group. Stress and fatigue were common tinnitus triggers across all ages, yet loud noise exposure was significantly more frequent among young patients. Comorbid conditions such as hyperacusis, headache, and dizziness were more prevalent in the young and middle-aged groups, while neck/jaw pain and psychiatric symptoms did not differ significantly across age groups.
Conclusion
Significant age-related differences exist in tinnitus characteristics and associated factors, particularly when comparing younger and older populations. These findings underscore the need for tailored, age-specific audiological assessments and treatment strategies for tinnitus patients.
서 론
이명이란 외부로부터의 청각 자극 없이 소리가 들리는 증상으로 이명의 발생 기전에는 말초 청각계, 청각 중추 신경계, 체성감각계, 변연계, 전전두엽 등 대뇌의 여러 영역들이 관여하지만 그 전체적인 메커니즘은 아직 완전히 규명되지 않았다. 이명의 발생에 관련된 요인에 따라 환자들은 다양한 형태의 이명을 경험하며 이러한 이질적인 속성을 고려하지 않은 연구들이 종종 상충된 결과를 보고하고 있다. 이명 환자에 대한 진단적 접근은 우선 청각학적 검사를 통해 환자의 청력 상태와 이명의 높낮이, 강도 등을 측정하고, 여러 설문을 이용하여 이명 발생과 관련된 요소 및 임상 양상을 조사하며, 이명으로 인한 장애를 정량화하는 평가를 포함한다. 이는 이명의 발생, 지속 및 악화와 관련된 다양한 요인을 종합적으로 이해하기 위한 필수적인 과정이다. 또한 하나의 치료법으로 모든 종류의 이명을 치료할 수 없다는 점(one size does not fit all)도 치료 계획 수립 시 반드시 고려해야 할 기본 조건이다. 따라서 개별 적용이 가능한 보다 효과적인 치료법 개발을 위해 이명 환자들을 구분할 수 있는 주요 인자를 규명하려는 연구가 필요한 상황이다[1].
이명 발생과 관련된 가장 널리 알려진 요인은 감각신경성 난청이며, 청각적 요인 외에도 두부 손상, 편두통, 목과 턱의 체성 장애, 스트레스, 피로, 우울증, 불면증, 불안과 같은 정신 심리적 문제들도 이명의 발생 및 악화에 깊이 관여하고 있다. 청력이 저하된 상태에서 살아가던 중에 극심한 스트레스나 신체적 질환을 겪은 후, 난청이 있는 귀에 새로운 이명이 발생하거나 기존의 이명이 악화되는 경우도 빈번히 관찰된다. 이러한 이유로 이명의 발생과 악화는 대개 단일 요인이 아닌 여러 요소가 복합적으로 작용하는 결과로 이해하여야 한다[2].
우리나라에서 이명의 유병률은 12세 이상 인구에서 약 19.7%로 보고되며, 이는 연령에 따라 증가하는 경향을 보인다. 이는 노화의 직접적인 영향보다 노화로 인한 청력 저하가 더 큰 원인일 가능성이 있으며, 젊은 환자들에서는 과도한 소음 노출이 주요 청각학적 원인으로 제시되고 있다[3-6].
연령에 따른 이명의 특성 변화에 대한 연구가 진행되어 왔지만, 대부분의 선행 연구는 이명의 크기나 장애 정도만을 비교하는 데 그치고 있어, 이명 관련 인자들에 대한 종합적인 연구는 아직 부족하며, 상충된 결과들로 인해 일관된 결론을 도출하지 못하고 있다[7-10]. 본 연구에서는 청각 손상이 비교적 심하여 난청에 따른 이명이 발생할 것으로 추정되는 장년 및 노년군과 청력이 상대적으로 잘 보존된 젊은 환자군 간의 이명 발생 관련 요인들과 증상 발현 양상에서의 차이를 검증하고, 적절한 진단적 접근 및 치료 방법 적용에 도움이 되는 정보를 제공할 목적으로 각 연령 그룹에서 이명의 특성이 어떻게 다르게 나타나는지를 조사하고자 한다.
대상 및 방법
대 상
2019년 1월부터 2021년 3월까지 3개월 이상 지속된 만성 이명을 주소로 본원 이비인후과를 방문한 환자들 중에서 중이 질환, 돌발성 난청, 메니에르병, 박동성 이명 및 근 경련성 이명 등 특정 원인에 의해 유발된 이명이 확실한 경우를 제외하고 이학적 검사, 청력 검사, 이명도 검사 및 설문지 작성을 모두 완료한 환자 439명(596귀)을 연구 대상으로 선정하여 후향적인 의무기록 조사를 시행하였다. 이 연구는 본원의 기관윤리심의위원회의 심의를 통과하였다(KNUH-2019-04-013-005).
연구 방법
청력 및 이명도 검사는 국제 표준 IOS 8253-1 기준을 만족하는 이중벽 방음실에서 동일한 1인의 청각사가 환자의 초진 시에 시행하였다. 기도 청력 검사(0.125-16 kHz) 및 골도 청력 검사(0.25-4 KHz)와 함께 이명주파수 및 강도의 매칭(tinnitus pitch and loudness matching)을 포함한 이명도 검사를 순음 청력 검사기(MADSEN Astera2; GN Otometrics, Copenhagen, Denmark)를 이용하여 시행하였다. 이명이 있는 귀에 대해 순음 청력 검사를 실시하여 16 kHz까지 총 13개 주파수(125 Hz, 250 Hz, 500 Hz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz, 8 kHz, 10 kHz, 12 kHz, 14 kHz, 16 kHz) 의 평균 청력 역치(pure tone average, PTA)를 측정하였다. 또한, 낮은 주파수 5개(0.125-2 kHz)의 평균 청력 역치(PTA low), 중간 주파수 4개(3-8 kHz)의 평균 청력 역치(PTA mid), 높은 주파수의 4개(10-16 kHz)의 평균 청력 역치(PTA high)도 산출하였다.
이와 함께 초진 시 시행된 이명 설문지를 통해 이명장애척도(Tinnitus Handicap Inventory, THI), 이명의 크기(loudness; 0-10점), 하루 중 이명이 들리는 시간(awareness; 0-100점), 이명으로 인한 괴로움(annoyance; 0-10점), 이명이 생활에 미치는 불편함(handicap; 0-10점)을 시각 척도화 지수(Visual Analog Scale, VAS) 형식으로 평가하였다. 추가적인 설문조사를 통해 이명이 발생했을 시기에 과도한 소음 노출, 스트레스, 피로감, 정신적 충격, 사고나 부상 등의 경험 여부를 확인하였다. 또한, 청각과민증, 두통, 어지럼증, 목의 근육이나 턱관절 이상, 정신심리적 증상 등의 동반 증상들도 함께 조사하였다.
연구 자료의 정규분포 검정 결과, 대상 환자들의 모든 변수값들이 비정규 분포를 보였기 때문에 연속형 변수의 비교를 위해 Kruskal-Wallis test를 사용하였고 범주형 변수를 비교하기 위해 Pearson’s chi-square test를 적용하였다. 유의한 차이를 보이는 변수들에 대해서는 다중 검정에 의한 위양성 판정을 피하기 위해 Bonferroni correction을 시행하였다. 또한, 연령과의 상관성 분석을 위해 연령과 연속형 변수 간에는 Spearman’s correlation, 연령과 범주형 변수 사이에는 point-biserial correlation을 실시하였다. 모든 통계 분석은 SPSS 소프트웨어 ver. 26.0 (IBM Corp., Armonk, NY, USA)를 사용하여 시행하였고 p<0.05인 경우를 통계적으로 유의한 차이가 있다고 판정하였다.
결 과
본 연구의 대상 총 439명(596 귀)을 연령에 따라 30세 이하 청년(young), 31-49세 중년(middle-aged), 50세 이상 장·노년(elderly)의 세 군으로 분류하였다. 청년군은 88명(21.0%), 중년군은 140명(31.9%), 장·노년군은 211명(48.1%)이었으며 각 군의 평균 나이는 청년군에서 21.8±5.0세, 중년군에서 40.4±5.4세, 장·노년군에서 64.2±8.9세로 나타났다. 성별 분포는 남성 186명(42.4%), 여성 253명(57.6%)이었다. 전체 주파수의 평균 청력 역치(PTA), 낮은 주파수 5개(0.125-2 kHz)의 평균 청력 역치(PTA low), 중간 주파수 4개(3-8 kHz)의 평균 청력 역치(PTA mid), 높은 주파수 4개(10-16 kHz)의 평균 청력 역치(PTA high) 모두에서 세 군 간에 유의한 차이가 있었다(p<0.05) (Table 1).
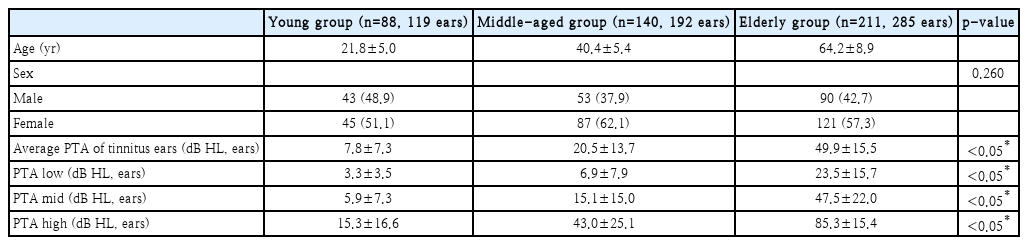
Demographic and audiological profiles of the three age groups
이명을 호소하는 귀의 좌, 우 및 양측 분포는 연령대별로 차이가 없었다. 이명의 이환 기간은 청년군에서 평균 16.3±27.1개월, 중년군에서 13.0±31.2개월, 장·노년군에서 35.0±64.1개월로 장·노년군에서 이명의 유병 기간이 가장 길었다(p<0.05). 이명 주파수는 청년군에서 평균 6.1±5.4 kHz, 중년군에서 5.6±4.9 kHz, 장·노년군에서 5.9±4.0 kHz로 세 군 간에 유의한 차이는 없었다. 이명도 검사에서 청력 역치를 보정한 이명의 크기(dB SL)는 청년군에서는 13.3±12.7 dB SL, 중년군에서는 9.9±7.3 dB SL, 장·노년군에서는 6.0±7.4 dB SL로 장·노년군에서 가장 작게 나타났다(p<0.05). 시각 척도화 지수(VAS)로 조사한 하루 중 이명이 들리는 시간(awareness)은 장·노년군이 다른 두 군보다 유의하게 길었으나(p<0.05), 이명으로 인한 괴로움(annoyance), 이명의 크기(loudness), 이명이 생활에 미치는 불편함(handicap), 그리고 이명장애척도(THI) 점수는 세 군 사이에 유의한 차이를 보이지 않았다(Table 2).
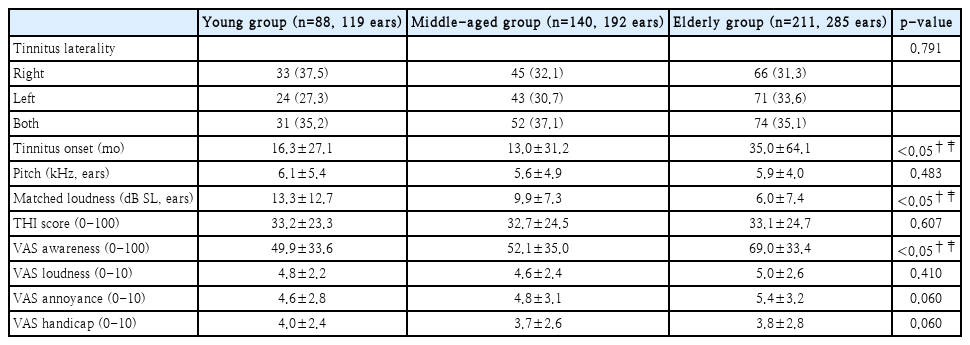
Comparison of tinnitus characteristics between the three age groups
이명의 발생과 관련된 증상들 중 큰 소리 노출만이 청년군에서 유의하게 더 자주 경험한 것으로 관찰되었다(p<0.05). 반면에 스트레스, 피로감, 정신적 충격, 사고나 부상과 관련해서는 세 군 간에 유의한 차이가 없었다(Table 3).
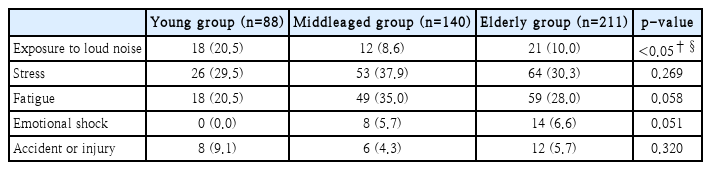
Associated factors with tinnitus development
동반 증상으로서 청각과민증, 두통 및 어지럼증은 청년군과 중년군이 장·노년군보다 유의하게 자주 보고하였으나(p<0.05) 청년군과 중년군 간에는 차이가 없었다. 한편, 목의 근육이나 턱관절의 체성 장애와 정신심리학적 증상의 유무는 세 군 간에 빈도 차이가 없었다(Table 4).
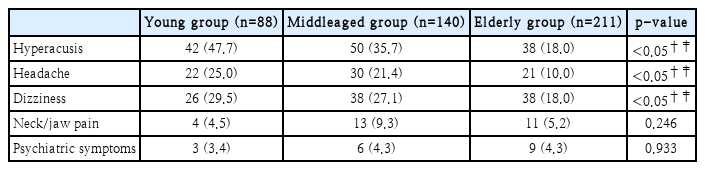
Comorbid symptoms of tinnitus in the three age groups
유의한 변수들과 연령 사이의 상관성(correlation) 결과, 이명의 크기(dB SL)가 상관계수 r=-0.34로 변수들 중 비교적 강한 음의 상관관계(젊을수록 큰)를 보였다(p<0.05). 또한, 이명을 느끼는 시간(awereness)은 r=0.28로 유의한 양의 상관성을 보였으며 큰소리 노출의 상관 계수는 r=-0.11, 청각과민증 r=-0.29, 두통 r=-0.18, 어지럼증은 r=-0.13, 모두 연령과 약한 음의 상관성을 나타냈다(p<0.05) (Table 5).
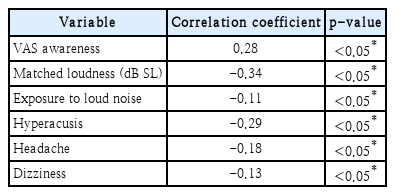
Correlation analysis of age-related factors
고 찰
본 연구에서는 439명의 만성 이명 환자를 세 연령군으로 분류하여 연령별 이명의 특성 차이를 포괄적이고 상세하게 분석하고자 하였다. 일반적으로 65세 이상을 노년군으로 분류하지만, 본 연구에서는 50-64세 장년군과 65세 이상의 노년군 간 청력 역치와 이명 유병 기간을 제외하고는 유의한 차이가 없어, 두 그룹을 장·노년군으로 통합하였다. 또한, 비교를 위해 대상 환자 수가 통계적으로 충분하고 이명의 다양한 특성을 종합적으로 분석한 선행 연구들만 선별하여 본 연구 결과와 비교해 보았다(Table 6).
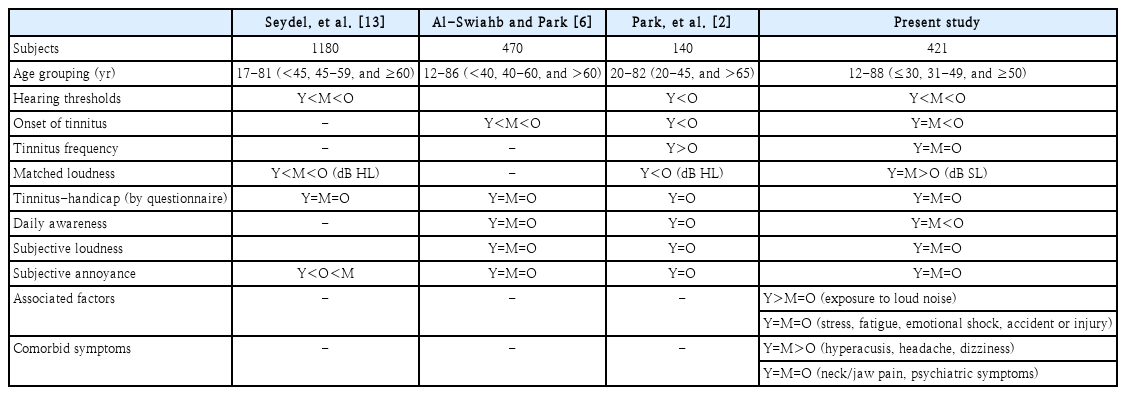
Summary of previous and present studies on age-related variations in tinnitus characteristics
청력 역치는 세 군 간 유의한 차이를 보였으며, 연령이 낮을수록 청력 역치도 낮았다. 고주파 영역까지 정상 청력을 유지하는 이명 환자는 주로 젊은 층에서 관찰되었으며, 이에 대해서는 순음청력검사로 확인되지 않는 외유모세포 손상이나 내유모세포와 청신경 섬유 사이의 시냅스 결손에 의한 와우 시냅스 질환(cochlear synaptopathy)이나 체성 장애, 정신 심리적 요인 등 비청각적 원인을 의심할 수 있다[11,12].
본 연구 결과, 장·노년군에서 이명 크기가 가장 작은 것으로 나타났다. 대부분의 선행 연구는 고령층에서 이명 크기(dB HL)가 더 크다고 보고하였으나, 본 연구에서는 젊은 두 군이 장·노년군보다 매칭한 이명 크기(dB SL)가 유의하게 큰 것으로 관찰되었다[2,13]. 본 연구는 청력 역치를 보정한 이명 크기를 sensation level로 측정한 결과, 오히려 젊은 환자들이 이명을 더 크게 느끼고 있음을 보여주었다.
이명 주파수와 난청 주파수 간 연관성에 대한 기존의 연구들은 이명 주파수와 청력 최대 손상 주파수 또는 난청이 시작되는 주파수(edge frequency) 사이에 연관성을 보고하거나 혹은 아예 연관성이 없다고 보고하기도 한다[14-17]. 이전 연구에 따르면, Park 등 [2]은 젊은 환자군에서 고령 환자군보다 이명 주파수가 더 높다고 보고하였으나, 본 연구에서는 세 군 모두 연령이나 청력 상태와 무관하게 평균 5-6 kHz의 유사한 이명 주파수를 기록하였다. 이는 난청이 시작되는 주파수가 연령과 상관없이 비슷하게 나타나기 때문일 것으로 추정된다.
여러 선행연구들에서와 마찬가지로 이명장애척도(THI) 점수, 이명으로 인한 괴로움(annoyance), 주관적인 이명의 크기(loudness), 이명이 생활에 미치는 불편함(handicap)의 시각 척도화 지수(VAS)는 세 군 사이에 유의한 차이를 보이지 않았다. 그러나 이명이 들리는 시간(awareness)은 장·노년군이 다른 두 군보다 유의하게 길었으며 이는 청력 역치가 높은 장·노년군에서 환경소음에 의한 이명 차폐가 부족하고, 사회 활동 시간도 상대적으로 짧아 이명 인지 시간이 길어진 것으 로 해석할 수 있다[10,18].
모든 군에서 스트레스와 피로가 20% 이상의 비율로 나타 나 공통적으로 이명 발생에 영향을 미치는 것으로 확인되었 다. 그러나 이명 발생 시 소음 노출은 청년군에서만 유의하게 높은 빈도로 관찰되어, 청력이 비교적 양호한 10-20대에서 소음 노출이 주요 원인임을 시사한다. 만성 소음 노출이 흔한 직업적 요인보다는 이어폰 과다 사용이나 군대 사격 훈련 등이 청년군에서 이명을 유발하는 주요 원인으로 추측된다[19,20]. 따라서 젊은 이명 환자에게는 소음 노출 병력을 확인하고, 청력 역치의 명확한 변화가 없더라도 미세 청각 손상이나 시냅스 결손 가능성을 확인하기 위해 이음향 방사 및 청성뇌간반응검사를 추가로 시행하는 것이 필요하다.
청각과민증은 모든 연령에서 이명과 함께 가장 흔히 나타나는 증상으로 확인되었으며, 청년군과 중년군에서 장·노년군보다 유의하게 높은 빈도를 보였다. 기존 연구에 따르면, 청각과민증이 동반된 이명 환자는 그렇지 않은 환자보다 나이 가 젊고, 청력 역치가 더 낮은 경향을 보였다[21].
본 연구에서 청년군 및 중년군은 두통과 어지럼증의 동반 비율이 높았다. 선행 연구에 따르면 다양한 유형의 두통에서 이명의 유병률이 높으며 Nowaczewska 등은 두통을 동반한 이명 환자들이 더 젊고 청력 역치가 더 낮다고 보고하였다[22,23]. 또한 Langguth 등[24]은 이명 환자의 약 45%가 두통을 함께 겪고, 주로 두통이 이명보다 먼저 발생한다고 밝혀 이명 과 두통 간 공통된 병리생리학적 기전의 가능성을 시사하였 다. 어지럼증을 동반한 이명 환자들은 우울감, 불안, 스트레 스 수준이 더 높고 이명장애척도(THI) 점수 또한 상승하는 경향을 보였다[25,26]. 이러한 결과는 특히 20-40대의 이명 환자에서 이러한 동반 증상들이 이명과 연관되어 정신적, 정서 적 상태에 부정적인 영향을 미칠 수 있다는 것을 시사한다. 따라서 병력 청취 시 이러한 신체적, 정서적 증상들을 함께 확인하여 종합적인 치료 계획을 세우는 것이 중요할 것이다.
목 근육이나 턱관절 이상의 체성 장애(somatosensory disorder)의 동반 비율은 세 군 간 유의한 차이를 보이지 않았다. 이명 환자에서 체성 장애의 동반 빈도는 34%-85%로, 주로 턱관절 장애(temporomandibular joint disorder)로 인한 경우가 많다[27]. 턱관절 장애는 45-64세 사이에서 가장 많고, 젊은 연령대와 노인층에서는 상대적으로 낮은 유병률을 보인다[28]. 본 연구에서 세 군의 발생 비율이 유사하게 나타난 것은 청년 이명 환자군에서 목 근육 및 턱관절 이상 빈도가 일반인보다 높을 수 있음을 시사한다. 턱관절 장애 환자들의 이명 발생 빈도는 그렇지 않은 환자들에 비해 8배 높고, 턱관절 장애를 동반한 이명 환자들이 이명만 있는 환자들보다 더 젊은 경향을 보였다[29-31]. 비록 세 군 간의 차이는 유의하지 않았지만, 턱관절 장애 치료가 이명 증상 개선에 도움이 되므로, 이명 환자에서 관련 이상 여부를 확인하는 것이 임상적으로 중요하다[32].
본 연구는 후향적 연구로서 보다 특화된 질문이나 검사를 시행하지 못했다는 한계가 있다. 연령이 어릴수록 청력 역치는 낮게 나타났지만 순음청력검사로는 확인되지 않는 외유모 세포의 미세한 손상이나 내유모세포와 청신경 섬유 사이의 시냅스 결손으로 발생할 수 있는 ‘숨겨진 난청(hidden hearing loss)’을 확인하기 위해서는 이음향방사검사와 청성뇌간 반응검사 등 추가적인 청력 검사가 필요하다. 또한 체성 장애에 대한 구체적 평가를 위해 근육의 압통 및 통증 유발점 유무, 근육 운동 범위 제한 등을 추가적으로 조사하고 이명의 체성 조절 검사를 시행하는 것도 고려할 수 있다. 또한, 우울이나 불안, 스트레스와 같은 정신심리학적 요인들을 객관적으로 평가하기 위해 적절한 지표를 사용한 추가 분석 또한 필요할 것이다.
본 연구는 연령에 따른 이명 발생 관련 요인과 발현 양상의 차이를 검증하고자 하였으며, 연령별 이명 환자 비교를 통해 이명의 특성을 조사하였다. 그 결과, 청년군 및 중년군에서 이명을 더 크게 느끼고, 청각과민증, 두통, 어지럼증과 같은 동반 증상이 더 자주 나타났으며, 특히 청년군에서 이명 발생 당시의 소음 노출 병력이 더 빈번하게 보고되었다. 이러한 연령에 따른 이명 발생 관련 요인과 발현 양상의 뚜렷한 차이를 고려할 때, 이명 환자 진료 시 포괄적인 청각 검사와 함께 비청각적 요인에 대한 충분한 조사가 필요하며, 연령별 특성을 반영한 진단 및 치료 접근법을 모색해야 할 것으로 판단된다.
Acknowledgements
None
Notes
Author contributions
Conceptualization: Ye-Sol Jung, Eui-Cheol Nam. Data curation: Ye-Sol Jung, Eui-Cheol Nam. Formal analysis: Ye-Sol Jung, Eui-Cheol Nam. Funding acquisition: Eui-Cheol Nam. Investigation: Ye-Sol Jung, Eui-Cheol Nam. Methodology: Ye-Sol Jung, Eui-Cheol Nam. Project administration: Eui-Cheol Nam. Resources: Eui-Cheol Nam. Software: Eui-Cheol Nam. Supervision: Eui-Cheol Nam. Validation: Ye-Sol Jung, Eui-Cheol Nam. Visualization: Ye-Sol Jung. Writing—original draft: Ye-Sol Jung. Writing—review & editing: Eui-Cheol Nam.