Metastatic Renal Cell Carcinoma Initially Presenting as a Laryngeal Mass: A Case Report
후두 종괴로 최초 발현된 전이성 신세포암 1예
Article information

Abstract
Tumors that metastasize to the larynx are extremely rare, accounting for less than 1% of all laryngeal malignancies. Although renal cell carcinoma (RCC) has a high metastatic potential, metastasis to the larynx is uncommon. Furthermore, it is exceptionally rare for a laryngeal metastasis to be the initial presentation of an undiagnosed RCC. We report a case of a 68-year-old female who presented with hoarseness. Preoperative laryngoscopy and imaging suggested a benign vascular tumor, such as hemangioma. However, surgical excision revealed a mass originating from the laryngeal ventricle, which was pathologically confirmed as metastatic clear cell RCC. Subsequent workup revealed a primary renal mass with adrenal metastases. This case highlights the importance of including metastatic carcinoma in the differential diagnosis of hypervascular laryngeal masses, even in patients without a known history of malignancy.
Introduction
Secondary carcinomas metastatic to the larynx are rare, accounting for approximately 0.09% to 0.4% of all malignant laryngeal tumors [1,2]. Melanoma and renal cell carcinoma (RCC) are the most common primary malignancies, followed by breast and lung cancers [3]. Among tumors originating in infraclavicular organs, RCC is known to have the highest frequency of laryngeal metastasis.
RCC is highly vascular and frequently metastasizes to almost any site in the body [4]. However, metastasis to the head and neck region, particularly the larynx, remains uncommon. Such lesions are usually detected during follow-up after an initial diagnosis of RCC. It is rare for a laryngeal mass to be the first clinical manifestation in a patient without a known history of malignancy [5]. In such cases, the lesion may be misdiagnosed clinically as a benign condition, such as a hemangioma or granuloma, requiring caution during the diagnostic and therapeutic process.
We report a case in which a patient presenting with hoarseness was initially suspected of having a hemangioma but was ultimately confirmed, only after surgical excision, to have laryngeal metastasis from a previously undiagnosed RCC. Laryngeal metastasis from RCC was first reported by Allan Fields [5] in 1966. Since then, only a small number of cases have been documented worldwide. In the Korean literature specifically, instances in which a primary malignancy is first diagnosed through a laryngeal metastasis are rarely reported. Therefore, we present this case alongside a literature review focusing on its clinical features and differential diagnosis.
Case
A 68-year-old female presented with persistent hoarseness for 4 months. She had experienced severe vomiting at symptom onset, but reported no associated dyspnea or dysphagia. Her medical history was unremarkable except for hypertension, and she had no smoking history.
Laryngoscopy and stroboscopy revealed a smooth, erythematous, pedunculated mass appearing to arise from the left false vocal fold. The mass covered the anterior commissure and bilateral supraglottis (Fig. 1), partially obstructing the glottic chink and interfering with vocal fold vibration. On preoperative auditory-perceptual assessment using the GRBAS scale, the patient scored G2R1B2S1, and the Voice Handicap Index-30 (VHI-30) total score was 42. Aerodynamic evaluation showed a maximum phonation time (MPT) of 9.79 seconds, a mean flow rate of 152 mL/sec, and a maximum subglottal pressure (Psub) of 11.48 cmH2O.
Preoperative laryngoscopic finding. A smooth, reddish, pedunculated mass is observed covering the anterior commissure and the left supraglottic area.
Contrast-enhanced neck CT demonstrated an approximately 9 mm markedly enhancing nodule in the midline, just superior to the anterior commissure. There was no evidence of tissue invasion or cartilage erosion. Radiologically, a paraganglioma or a hypervascular tumor was suspected (Fig. 2). On dynamic contrast-enhanced laryngeal MRI, early-phase enhancement was minimal, whereas delayed-phase enhancement was conspicuous. This delayed enhancement pattern suggested a benign vascular lesion, such as a venous malformation or cavernous hemangioma (Fig. 3).
Preoperative neck CT findings. Contrast-enhanced CT images in (A) coronal and (B) axial views show a markedly enhancing nodule (arrows) measuring approximately 9 mm in the midline supraglottic area, just above the anterior commissure. There is no evidence of cartilage erosion or invasion into surrounding deep tissues, suggesting a hypervascular tumor.
Preoperative Larynx MRI findings. (A) Axial T2-weighted turbo spin-echo image with Dixon fat suppression shows a hyperintense lesion in the supraglottic area. (B) An early-phase dynamic contrast-enhanced axial 3D T1-weighted gradient-echo (VIBE) image with fat suppression reveals minimal enhancement, whereas (C) a delayed-phase axial T1-weighted turbo spin-echo (TSE) image with Dixon fat suppression demonstrates significant enhancement. This delayed enhancement pattern suggested a vascular lesion, such as a cavernous hemangioma or venous malformation.
Suspension laryngoscopic microsurgery was performed under the presumptive diagnosis of a benign vascular tumor. Because there was a risk of tumor bleeding during endotracheal intubation, the patient and her family were informed in advance about the possibility of a tracheostomy under local anesthesia if needed, and consent was obtained. Fortunately, the anesthesiologist achieved safe endotracheal intubation without tumor injury, and the operation proceeded as planned without a tracheostomy.
During surgery, retraction of the mass revealed its true origin within the left laryngeal ventricle, contrary to the preoperative endoscopic impression of the anterior commissure. Because adequate visualization of the deep origin was difficult with suspension laryngoscopy alone, a partial resection of the left false vocal fold was first performed using a KTP laser (2 Watt, continuous mode) to secure the operative field. Complete excision of this highly vascular tumor and simultaneous hemostasis of the stalk were then achieved using the KTP laser (6 Watt, 50 ms/150 ms, pulsed mode). Compression hemostasis was applied for 10 minutes with a 1:10000 epinephrine pledget, after which no further bleeding was observed. The estimated blood loss was minimal at approximately 20 mL. After approximately 6 hours of observation in the ambulatory surgery center, the patient was safely discharged without airway or bleeding complications.
Histopathological examination of the specimen demonstrated a clear cell neoplasm. On immunohistochemical staining, the tumor cells were positive for CD10, PAX8, and CA9 (Carbonic Anhydrase IX), and negative for neuroendocrine markers including Chromogranin, Synaptophysin, and INSM1 (Fig. 4). The resected false vocal fold tissue showed chronic inflammation.
Histopathological findings of the laryngeal tumor. (A) Hematoxylin and eosin staining demonstrates tumor cells with abundant clear cytoplasm arranged in compact nests and sheets, separated by thin-walled sinusoidal vascular channels. Tumor nuclei are round to oval with prominent nucleoli (Scale bar=100 μm). Immunohistochemical staining shows: (B) CD10—diffuse, strong (3+) granular cytoplasmic and membranous positivity throughout the tumor nests, with no staining in surrounding stromal or vascular cells; (C) PAX8—diffuse, moderate-to-strong (2–3+) nuclear positivity, with clean, dot-like brown chromogenic signal confined to tumor cell nuclei and no appreciable cytoplasmic background; (D) CA9 (Carbonic Anhydrase IX)—diffuse, strong (3+) circumferential membranous positivity in a “chicken-wire” pattern, characteristic of hypoxia-driven expression in clear cell renal cell carcinoma, with sparing of intratumoral necrotic areas. These immunohistochemical findings are consistent with metastatic clear cell renal cell carcinoma.
Postoperative laryngoscopy confirmed complete excision of the lesion, with only focal fibrosis remaining in the left supraglottis (Fig. 5). Postoperatively, voice parameters showed overall improvement, with the GRBAS scale score improving to G1R1B1S1 and the total VHI-30 score decreasing to 18. On aerodynamic assessment, the MPT increased to 11.92 seconds, the mean flow rate decreased to 121 mL/sec, and the Psub decreased to 9.92 cmH2O.
Postoperative laryngoscopic finding. The image shows complete removal of the mass with focal fibrosis on the left supraglottis. No evidence of local recurrence is observed.
The final diagnosis was metastatic clear cell RCC. Abdominal imaging performed to evaluate the primary site revealed an 11.1 cm mass in the left kidney along with bilateral adrenal metastases. The patient was transferred to the department of urology and underwent a robot-assisted radical nephrectomy followed by an adrenalectomy. Final histopathological examination of the resected kidney confirmed Fuhrman grade III clear cell RCC (T3aN0M1, Stage IV), and metastasis was also confirmed in both adrenal glands. She is currently under follow-up without systemic therapy.
Discussion
RCC is a urologic malignancy with a poor prognosis, and approximately 25% to 30% of patients have distant metastasis at the time of diagnosis [6,7]. The major metastatic sites include the lungs, lymph nodes, bones, and liver. Head and neck metastases account for 8% to 15% of all metastatic RCC cases. Laryngeal metastasis is considered rare because of the anatomical characteristics of the lymphatic and vascular circulation [1]. The proposed mechanisms of laryngeal metastasis from RCC include arterial spread through the systemic circulation and retrograde venous spread through Batson’s venous plexus. Batson’s venous plexus provides a route by which increased thoracoabdominal pressure causes retrograde flow into the vertebral venous system, allowing tumor cells to reach the head and neck region without pulmonary filtration [8-10]. In the present case, an event associated with increased intra-abdominal pressure, such as the severe vomiting reported at symptom onset, may have been related to this retrograde metastatic pathway. However, preoperative whole-body PET-CT showed no increased bony uptake suggestive of spinal metastasis.
Clinically, metastatic RCC of the larynx is difficult to distinguish grossly from benign conditions such as pyogenic granulomas, hemangiomas, and paragangliomas due to its inherent hypervascularity. In the present case, a hemangioma was strongly suspected preoperatively because CT and MRI showed strong enhancement and a delayed enhancement pattern. This diagnostic confusion increases the risk of unexpected massive bleeding during surgery. The key considerations for the differential diagnosis of these vascular laryngeal lesions are summarized in Table 1. In our case, the lesion was removed safely by identifying its origin within the laryngeal ventricle and performing a partial resection of the false vocal fold using a KTP laser, which is useful for the resection of vascular tumors.
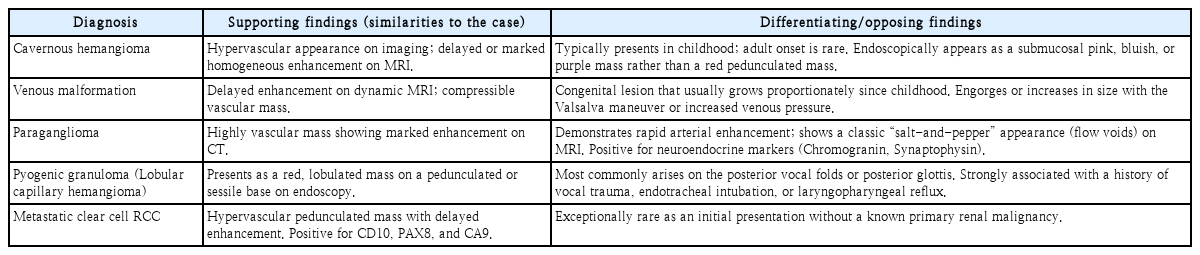
Differential diagnosis of hypervascular laryngeal lesions
Histopathological examination and immunohistochemical staining are essential for a definitive diagnosis. The differential diagnosis includes the clear cell variant of primary laryngeal squamous cell carcinoma and neuroendocrine tumors [11]. RCC typically shows positivity for vimentin and CD10. In particular, the expression of PAX8 and CA9 provides important evidence of a renal origin [1,2,12]. In this case, positive staining for these markers confirmed the diagnosis of RCC.
The treatment of metastatic RCC is determined based on the patient’s general condition and the pattern of metastasis. While the prognosis has historically been poor, recent studies suggest that aggressive surgical resection for solitary or oligometastatic disease may offer survival benefits [13,14]. Furthermore, advances in targeted therapies and immunotherapies have been associated with improved survival rates over the past decade [15]. This case is notable for the rare clinical presentation of an asymptomatic primary RCC initially manifesting as a laryngeal metastasis. It underscores the importance of including metastatic disease in the differential diagnosis of vascular laryngeal masses to facilitate early diagnosis and appropriate surgical intervention.
Supplementary Materials
Korean translation of this article is available with the Online-only Data Supplement at https://doi.org/10.3342/kjorl-hns.2026.00038.
Notes
Acknowledgments
This case report was granted an exemption from review by the Institutional Review Board of Seoul St. Mary’s Hospital, The Catholic University of Korea (No. KC26ZASI0026). Written informed consent for the publication of the patient’s clinical information and photographs was also obtained from the patient.
Author Contribution
Conceptualization: Oh-Hyeong Lee. Data curation: Ji-Woo Kim, Kyung-gyu Yeom, Hee-su Yoon. Formal analysis: Ji-Woo Kim, Oh-Hyeong Lee. Investigation: all authors. Methodology: Oh-Hyeong Lee. Project administration: Oh-Hyeong Lee. Resources: Oh-Hyeong Lee. Supervision: Oh-Hyeong Lee. Validation: Oh-Hyeong Lee. Visualization: Ji-Woo Kim. Writing—original draft: Ji-Woo Kim. Writing—review & editing: Oh-Hyeong Lee, Ji-Woo Kim.