Validation of the Korean Version of the “Empty Nose Syndrome 6-Item Questionnaire (ENS6Q)”
빈코증후군 6문항 설문도구의 한국어판 타당성 검증
Article information

Abstract
Background and Objectives
Empty nose syndrome (ENS) is difficult to diagnose because objective findings often do not correlate with symptom severity. The Empty Nose Syndrome 6-item Questionnaire (ENS6Q) has been developed to assess ENS-specific symptoms, but there has not been sufficient verification research for a Korean version.
Subjects and Method
A Korean version of the ENS6Q (ENS6Q-KAV) was administered twice to patients with ENS, normal controls, and patients with chronic rhinosinusitis (CRS). Known-groups validity was evaluated using the Kruskal-Wallis test followed by the Bonferroni-corrected post-hoc analyses. Reliability was assessed using Cronbach’s α and the intraclass correlation coefficient [ICC(3,1)]. Diagnostic accuracy was evaluated using the receiver operating characteristic (ROC) analysis.
Results
ENS6Q-KAV total scores differed significantly among the three groups at both administrations (H=57.86 and 61.34, respectively; p<0.001), with the ENS group showing significantly higher scores than both the normal control and CRS groups. All item scores were also significantly higher in the ENS group (adjusted p<0.001). Internal consistency was high (Cronbach’s α=0.861-0.884), and test-retest reliability was excellent (ICC=0.937; 95% confidence interval, 0.914-0.955). ROC analysis demonstrated excellent discrimination between ENS and normal controls (area under the curve [AUC]=0.948-0.962) and robust discrimination between ENS and CRS (AUC=0.915-0.931), with an optimal cut-off score of 9.
Conclusion
The ENS6Q-KAV is a reliable and valid tool for assessing ENS-specific symptoms and effectively distinguishes ENS from normal controls and CRS in Korean-speaking patients.
Introduction
Empty nose syndrome (ENS) was first described by Eugene Kern in 1994 and is known as a rare iatrogenic disorder that develops after turbinate resection or reduction surgery [1]. Increased nasal cavity volume and the resulting changes in nasal airflow lead to reduced mucosal sensation and atrophy. Patients complain of subjective symptoms such as paradoxical nasal obstruction, nasal dryness, pain, crusting, and a sensation of heat. However, these symptoms are not adequately explained by conventional objective examinations such as endoscopy or imaging studies, and the diagnosis of ENS therefore remains a clinical challenge.
Questionnaires currently used in clinical practice, including the Visual Analogue Scale, Nasal Obstruction Symptom Evaluation, and Sino-Nasal Outcome Test-22, are useful for assessing the overall severity of sinonasal symptoms. However, they do not adequately reflect the distinctive and distressing abnormal sensations and psychological discomfort experienced by patients with ENS. To more accurately capture the symptom specificity of ENS, Nayak, et al. developed the Empty Nose Syndrome 6-item Questionnaire (ENS6Q), which has been reported to be a reliable and valid tool for aiding the diagnosis of ENS [2].
Since then, the ENS6Q has been translated into several languages, including German, and its cultural and linguistic validity has been established in these translated versions (ENS6Q-GAV) [3]. However, systematic validation studies of a Korean version are still lacking. In particular, validation of its discriminative ability against not only healthy controls but also patients with chronic rhinosinusitis (CRS) who complain of nasal discomfort has been limited.
Therefore, the aim of this study was to develop a Korean version of the ENS6Q (ENS6Q-KAV) and to evaluate its validity, reliability, and diagnostic utility through a three-group comparison including patients with ENS, healthy controls, and patients with CRS. In addition, we sought to examine test-retest reliability through repeated administration of the questionnaire and to assess diagnostic accuracy using receiver operating characteristic (ROC) analysis.
Subjects and Methods
This study was conducted from September 2025 to November 2025. Given the rarity of the disease, the eligible age for study participation was set at 17 years or older. Individuals aged 17 years were included only when they were considered capable of understanding the questionnaire items and responding voluntarily. All participants were enrolled after receiving a sufficient explanation of the study and completing the informed consent process. This study was approved by the Institutional Review Board of Kosin University Gospel Hospital (IRB No. KUGH 2018-12-026-008).
The ENS6Q consists of six items. Each item is scored on a 6-point scale ranging from 0, corresponding to “not at all,” to 5, corresponding to “very severe.” First, the original English ENS6Q was translated into Korean by two board-certified otorhinolaryngologists. The translated version was then reviewed together with another bilingual otorhinolaryngologist fluent in Korean and English, and consensus was reached regarding vocabulary, grammar, and cultural appropriateness. It was subsequently back-translated into English by two bilingual Korean-English speakers and one professional English translator/interpreter, and semantic equivalence was confirmed. Approval was then obtained from Nayak JV, the developer of the ENS6Q. Finally, after questionnaire completion, interviews were conducted with five patients with ENS and five healthy individuals regarding item comprehension, ambiguous expressions, and terminology difficulty. After reflecting the suggested revisions, the final Korean questionnaire, ENS6Q-KAV, was established (Fig. 1).
A: Original English version of Empty Nose Syndrome 6-item Questionnaire (ENS6Q). B: Korean version of Empty Nose Syndrome 6-item Questionnaire (ENS6Q-KAV).
For the study, participants were divided into three groups: an ENS group, a healthy control group, and a CRS group. The ENS group consisted of individuals with a history of inferior turbinate resection or reduction surgery, objective structural defects identifiable on endoscopy or CT, complaints of discomfort related to the nasal mucosa and nasal breathing, and a positive Cotton test, defined as symptom improvement when the structural defect site was augmented with a cotton ball. Individuals aged 16 years or younger, those with sinusitis, and those who could not understand Korean were excluded.
Healthy controls were recruited from volunteers aged 17 years or older with “healthy noses.” They had no history of nasal or paranasal sinus surgery, had no sinonasal disease at the time of the survey, and were able to sufficiently understand and read Korean.
The CRS group was diagnosed according to international clinical practice guidelines. Specifically, CRS was defined as the presence of at least two symptoms among nasal obstruction, rhinorrhea, facial pain, or reduced olfaction persisting for more than 12 weeks, together with either purulent discharge, mucosal edema, or nasal polyps on nasal endoscopy, or mucosal thickening or increased opacification on paranasal sinus CT.4) All patients underwent nasal endoscopy and radiologic evaluation before study participation, and enrollment was based on these objective findings. However, patients with a prior history of sinonasal surgery or procedures were excluded.
Participants completed the questionnaire twice within an interval of 2 weeks after the first survey. After questionnaire administration, their understanding of the six ENS6Q-KAV items was then confirmed.
To compare ENS6Q-KAV scores among the three groups, the nonparametric Kruskal–Wallis test was used. For post hoc analysis, pairwise Mann–Whitney U tests with Bonferroni correction were applied. Internal consistency of the questionnaire was assessed using Cronbach’s α, and test-retest reliability was analyzed using the intraclass correlation coefficient [ICC(3,1)] based on a two-way mixed-effects model with absolute agreement. Diagnostic accuracy was evaluated using ROC curve analysis, and the area under the curve (AUC), the optimal cutoff value based on the Youden index, sensitivity, and specificity were calculated. All statistical analyses were performed using a two-tailed test, and statistical significance was defined as p<0.05. Statistical analyses were conducted using SPSS version 22.0 (IBM Corp.).
Results
A total of 143 participants were included in the analysis, comprising 32 in the ENS group, 67 in the healthy control group, and 44 in the CRS group. The mean age was 40.22±2.83 years in the ENS group, 29.67±1.43 years in the healthy control group, and 59.02±2.02 years in the CRS group. A chi-square test was performed to compare sex distribution among the three groups, and no significant difference was found among the ENS, healthy control, and CRS groups (χ2(2)=1.59, p=0.451) (Table 1).
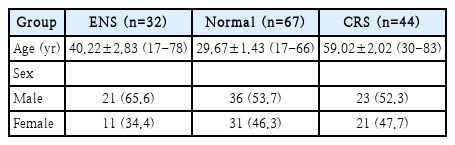
Demographic characteristics
Each item of the ENS6Q-KAV is scored from 0 to 5, with a total score ranging from 0 to 30, and higher scores indicate more severe symptoms. The total score did not follow a normal distribution on the Shapiro-Wilk test (first survey p=1.34 ×10-9, second survey p=6.02×10-11). Therefore, nonparametric tests were used for between-group comparisons (Table 2).
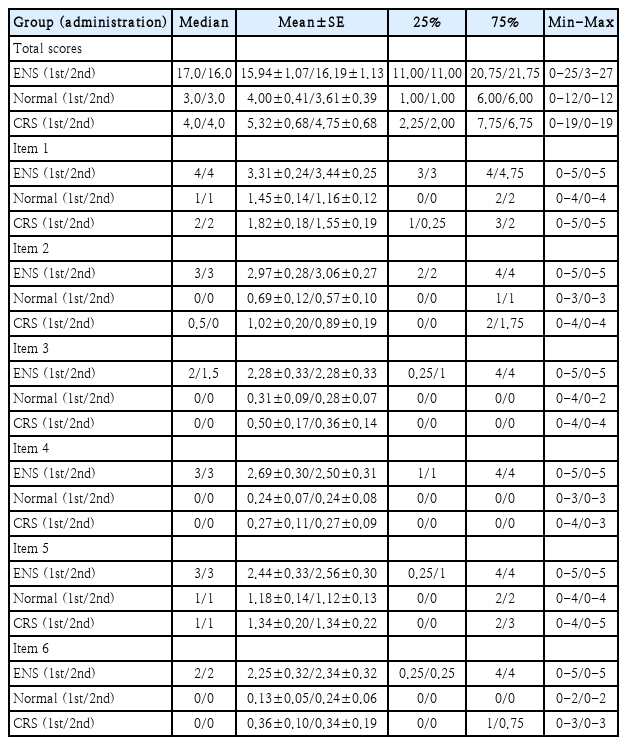
Descriptive statistics of ENS6Q-KAV total and item scores by group and administration
To evaluate the discriminative ability of ENS6Q-KAV scores among the three groups, the Kruskal–Wallis test was used. For post hoc analysis, pairwise Mann–Whitney U tests with Bonferroni correction were applied. Questionnaire scores differed significantly among the three groups in both the first survey (H=57.86, p<0.001) and the second survey (H=61.34, p<0.001), with the ENS group showing significantly higher scores than the healthy control and CRS groups. Analysis of individual item scores also showed that the ENS group had significantly higher scores than the healthy control and CRS groups (p<0.001) (Table 3). In the Bonferroni-corrected post hoc analysis, the ENS group differed significantly from both the healthy control group and the CRS group (p<0.05), whereas no significant differences were observed between the healthy control and CRS groups in either the total score or the item-level scores.
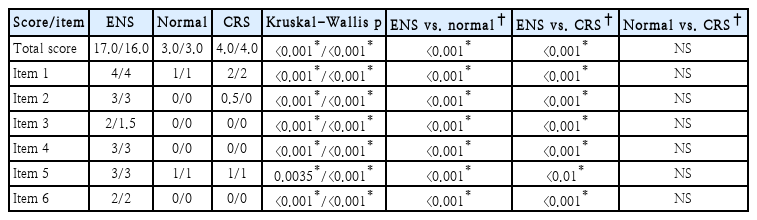
Known-groups validity of ENS6Q-KAV total and item scores among ENS, normal control, and CRS groups (median, 1st/2nd administration)
Internal consistency was assessed using Cronbach’s α to determine whether each ENS6Q-KAV item measured ENS symptoms consistently. Cronbach’s α was 0.861 in the first survey and 0.884 in the second survey, indicating high internal consistency.
Test-retest reliability, assessed to determine agreement between the first and second survey administrations, was evaluated using ICC(3,1), based on a two-way mixed-effects model with absolute agreement. The confidence interval (CI) was calculated as a 95% CI using the F distribution based on analysis of variance. The ICC for the total score was 0.937 (95% CI 0.914-0.955), indicating excellent test-retest reliability. Test-retest reliability was also evaluated for the individual items, and the ICC values for each item ranged from 0.81 to 0.92, indicating good to excellent reliability (Supplementary Table 1).
In ROC analysis performed to evaluate how well the ENS6Q-KAV total score discriminated the presence of ENS, the ENS and healthy control groups were distinguished with excellent accuracy, with AUC values of 0.948 and 0.962 in the first and second surveys, respectively. In the comparison between the ENS group and the CRS group, the AUC values were 0.915 and 0.931 in the first and second surveys, respectively, indicating good discriminative ability (Fig. 2). The optimal cutoff value based on the Youden index was 9 points in both comparisons. For the comparison between the ENS group and the healthy control group, the sensitivity was 93.8% and 90.6%, and the specificity was 85.1% and 92.5% in the first and second surveys, respectively. For the comparison between the ENS group and the CRS group, the sensitivity was 93.8% and 90.6%, and the specificity was 81.8% and 88.6% in the first and second surveys, respectively (Table 4).
ROC curves of the ENS6Q total score at the first (solid line) and second (dashed line) administrations. A: Discrimination of patients with ENS from normal controls (AUC=0.948 and 0.962, respectively). B: Discrimination of patients with ENS from patients with CRS (AUC=0.915 and 0.931, respectively). ROC, receiver operating characteristic; ENS6Q, Empty Nose Syndrome 6-item Questionnaire; CRS, chronic rhinosinusitis; AUC, area under the curve.
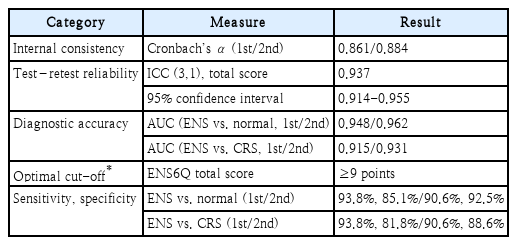
Reliability and diagnostic performance of the ENS6Q-KAV
Discussion
ENS is characterized by paradoxical nasal obstruction, in which patients subjectively complain of a suffocating sensation despite an adequately patent nasal cavity. Previous studies have repeatedly noted that objective diagnosis is extremely difficult. One reason is that nasal resistance does not necessarily correspond to patients’ subjective perception of breathing. In addition, nasal breathing discomfort has been reported to be more closely associated with reduced trigeminal sensation than with actual airflow resistance [5,6]. However, these functional abnormalities cannot be objectively demonstrated by conventional imaging modalities such as endoscopy or CT.
A second reason is that the symptoms reported by patients are understood as a sensory-neural disorder in which neurologic and hemodynamic abnormalities of the nasal mucosa act in combination. Accordingly, the symptoms are difficult to explain on the basis of anatomic defects alone. Because ENS can be diagnosed only after other possible causes have been excluded because of these complex sensory abnormalities, the objectivity of diagnosis is inevitably limited [6,7]. Third, patients experience not only physical symptoms but also psychological and psychiatric symptoms. Previous studies have reported that their quality of life is markedly lower than that of patients with other rhinologic diseases [8,9], and we have previously reported, using the Beck Depression Inventory-II (BDI-II), that more than half of these patients met the criteria for clinical depression [10]. T his depressive state is more closely associated with a reduced sense of control or autonomy in life than with nasal breathing difficulty itself [9].
In the present study, we evaluated the validity and reliability of ENS6Q-KAV, the Korean version of the ENS6Q, through a three-group comparison including patients with ENS, healthy controls, and patients with CRS. Both the total ENS6Q-KAV score and all item scores were significantly higher in the ENS group than in the healthy control and CRS groups in both the first and second surveys. No significant differences were observed between the healthy control and CRS groups. These findings suggest that ENS6Q-KAV is not merely a questionnaire reflecting the severity of general nasal symptoms, but rather a tool that effectively captures the subjective symptom burden specific to ENS.
The similar score distributions in the CRS and healthy control groups are of particular clinical importance. Although both ENS and CRS can cause nasal discomfort, their pathophysiologic mechanisms are fundamentally different. Our findings support that ENS6Q-KAV is better suited to distinguishing the sensory abnormalities and breathing discomfort characteristic of ENS than to reflecting symptom severity in inflammatory sinonasal disease.
In the reliability analysis, ENS6Q-KAV showed high internal consistency, with Cronbach’s α values of 0.861-0.884, and the test-retest reliability of the total score was excellent, with an ICC of 0.937. In addition, the item-level ICC values ranged from 0.81 to 0.92, indicating mostly good to excellent reproducibility. These findings indicate that responses to the questionnaire remained stable over time and suggest that ENS6QKAV has sufficient reproducibility for clinical use.
In the ROC analysis, the ENS6Q-KAV total score discriminated both the ENS and healthy control groups and the ENS and CRS groups with high accuracy. Notably, the optimal cutoff value was 9 points in both comparisons, suggesting a consistent and practical threshold for identifying patients with suspected ENS in clinical practice. These findings indicate that ENS6Q-KAV may serve as a useful adjunctive tool for the diagnosis of ENS in real-world clinical settings.
There were differences in age distribution among the three groups in this study. However, ENS6Q-KAV scores appear to have been influenced more by the presence of ENS than by age. Despite differences in age distribution, the healthy control and CRS groups showed no significant differences in either the total ENS6Q score or the item-level scores. This finding suggests that age itself is unlikely to be a major determinant of questionnaire scores. The ENS6Q was designed to assess ENS-specific subjective symptoms, such as paradoxical nasal obstruction, nasal dryness, and a sensation of heat, that occur after turbinate surgery. These symptoms are more closely related to surgical history and abnormal nasal sensation than to age. Nevertheless, the possibility that age may partially influence symptom perception or response patterns cannot be completely excluded. Future studies should therefore include further validation using multivariable analyses adjusted for age or cohorts with a more balanced age distribution.
In addition, the possibility cannot be excluded that conservative treatment administered in some patients during the interval between the two surveys may have affected score variation. However, because no procedural treatment was performed during the interval of less than 2 weeks other than routine nasal irrigation or ointment application that patients were already using, conservative treatment is unlikely to have had a major influence. It is also necessary to consider the possibility that environmental or psychological factors may have affected the reproducibility of certain items.
Nevertheless, this study systematically demonstrated that ENS6Q-KAV is a questionnaire with established reliability and validity in Korean-speaking users and suggests that it can be used as a clinically useful tool for the diagnosis of ENS [11]. In addition, in future work, we plan to establish a scientific basis for a multidimensional assessment framework by combining ENS6Q-KAV with patients’ psychological indicators assessed using the BDI-II that we previously reported.
Supplementary Materials
Korean translation of this article is available with the Online-only Data Supplement at https://doi.org/10.3342/kjorl-hns.2026.00017.
The Supplement is available with this article at https://doi.org/10.3342/kjorl-hns.2026.00017.
Notes
Acknowledgments
None
Author Contribution
Conceptualization: Jooyeon Kim, Jae Hwan Kwon. Data curation: Sue Jean Mun, Joo Hyun Lee. Formal analysis: Jooyeon Kim, Joo Hyun Lee. Investigation: Sue Jean Mun, Joo Hyun Lee. Methodology: Jooyeon Kim. Project administration: Jooyeon Kim, Jae Hwan Kwon. Resources: Sue Jean Mun, Joo Hyun Lee. Software: Jooyeon Kim, Jaebum Koh, Suhbin Kim. Supervision: Jooyeon Kim, Jae Hwan Kwon. Validation: Jooyeon Kim. Visualization: Sue Jean Mun, Joo Hyun Lee. Writing—original draft: Jooyeon Kim. Writing—review & editing: Jooyeon Kim, Jae Hwan Kwon.