혀에 발생한 랑게르한스 세포 조직구증: 증례 보고 및 문헌 고찰
Abstract
Langerhans cell histiocytosis (LCH) is commonly characterized by abnormal function and differentiation or proliferation of monocytes. In LCH, granulomatous lesions, including langerine- positive histocytes and inflammatory infiltrates, can occur at all tissues, particularly the bones, skin, lungs, and pituitary gland. Thirty nine-year-old male patient visited outpatient clinic with a mass on his tongue that had been presented one month prior. The initial size was 2×1.5 cm, but it gradually grew larger. The authors performed an incisional biopsy under local anesthesia, and the pathological diagnosis confirmed that LCH of the tongue. Several studies including bone marrow biopsy were performed to assess involvement of other organs. These tests show that only the tongue was involved in this case. The patient underwent further treatment with low-dose radiotherapy. We present this case of tongue LCH with a review of the literature.
Key words: Hematology ㆍ Langerhans cell histiocytosis ㆍ Tongue
서 론
랑게르한스 세포 조직구증(Langerhans cell histiocytosis, LCH)은 소아에서 흔하고, 매년 백만 명당 4-5명의 소아(0-15세)에서 진단된다[ 1, 2]. LCH는 호산구, 림프구, 호중구 및 거대 세포와 혼합된 랑게르한스 세포의 증식을 특징으로 하고[ 3], 단일 기관 침범에서 다기관 질환에 이르는 광범위한 임상 증상을 특징으로 하는 희귀 질환이다[ 4]. 주로 뼈, 피부, 뇌하수체, 간, 비장, 조혈기관, 폐, 림프절 및 중추 신경계(뇌하수체 제외)를 침범하고[ 5], 두경부에 발생하는 경우는 드물다. 앞선 문헌 보고에 따르면, 두경부에서 발생한 증례의 경우 측두골에 생긴 증례 보고는 있으나 혀를 침범한 사례는 없었다[ 1, 6]. 이에 LCH가 단일기관인 혀를 침범한 사례가 국내에 아직 없는 바 증례 보고 및 문헌 고찰을 하고자 한다.
증 례
39세 남자 환자가 한달 전부터 발생한 혀의 비압통성 종물을 주소로 본원 외래에 내원하였다. 혀의 앞쪽부분에 좌측 가장자리부터 중간까지 만져지는 약 2×1.5 cm 크기의 종물이었고 혀의 점막은 정상 소견을 보였다. 경부 촉진에서는 특이소견은 보이지 않았다( Fig. 1A). 환자는 조음기능, 연하기능에 장애를 호소하지는 않았고 혀의 감각 및 미각도 정상을 보였으나, 점차 커지는 양상의 종물로 인해 불편함을 호소하였다. 종물을 덮고 있는 점막이 정상 소견을 보였기 때문에 혈관 기원의 종물 또는 신경초종, 신경섬유종, 평활근종과 같은 양성종물을 우선 고려하여 감별을 위해 자기공명영상(MRI) 촬영을 진행하였다. 신경초종의 경우 MRI에서 일반적으로 T1 강조영상에서 저신호강도, T2 강조영상에서 고신호강도를 보이는 경계가 명확한 종물로 확인되는 반면, 본 환자의 경우 T1, T2 강조영상 모두에서 고신호강도를 보였고, 촉진에서는 경계가 명확한 부드러운 종물로 만져졌음에도 불구하고 영상에서는 경계가 불명확한 깊이가 1.8 cm에 이르는 악성 소견을 시사하였다( Fig. 2). 이에 조직학적 확인을 위해 국소마취하 절개 생검을 계획하였다. 정상 점막으로 덮힌 종물로 절개해보니 뚜렷한 경계가 없이 혀의 근육층에 침투된 황색의 육아종성 조직이 확인되었다. 병리검사에서 침윤된 랑게르한스 세포가 호산구와 함께 증식한 소견이 관찰되었고, 조직화학염색에서 S-100, CD1a, CD68에서 모두 양성을 보이며 LCH로 진단되었다( Fig. 3). 환자는 LCH의 다기관 침범 정도를 확인하기 위해 전신 양전자방출단층촬영(PET)을 비롯하여 골수검사 및 소화기 내시경을 진행하였고 모두 정상 결과를 보였으며 혀 이외의 다른 기관에서의 병변은 관찰되지 않았다. 검사 결과에 대해 이비인후과, 혈액종양내과, 종양내과, 방사선종양학과가 모여 다학제 진료를 진행하였다. 논의결과 Histiocyte Society의 치료지침에 기반하여 단일기관 병변으로 전신 항암치료보다는 국소치료인 수술적 절제 혹은 방사선치료를 고려하였다. 결과적으로 환자는 저용량 방사선치료(2800 cGy)를 받았고, 그 결과 방사선 종료 후 6개월째 시행한 PET에서 재발 소견은 없었으며, 현재 치료 종료 후 1년째 재발 없는 상태로 유지되고 있다( Fig. 1B).
고 찰
LCH는 주로 소아에서 발병하는 질환으로, 문헌에 따르면 67.9%가 18세 미만에서 발병한다고 알려져 있고, 남녀 비는 1.15:1로 남아에서 더 호발한다[ 7]. 임상징후는 자연적으로 관해가 될 수 있는 단일기관 침범에서부터 사망으로 이어질 수 있는 전신적이고 공격적인 양상까지 다양하게 나타날 수 있다. 전신의 모든 기관이 단독 또는 다기관으로 침범 가능하며 주로 뼈와 피부에서 더 높은 빈도로 관찰된다[ 8]. 이렇듯 LCH가 다양한 임상양상을 보이기 때문에 특히 성인의 경우 혈액 내과 전문가가 아닌 임상의사의 판단하에 부적절한 치료를 받게 되는 경우가 초래 될 수 있다[ 9, 10]. 성인의 경우 뚜렷한 표준 치료 요법이 없으며 성인을 모집단으로 한 전향적 시험이 시행된 바 없으며, 다양한 임상양상만큼 치료 또한 침범된 기관 및 그 침범 범위에 따라 다양해진다. LCH는 단일계통(single-system LCH, SS-LCH) 혹은 다중계통(multisystem LCH, MS-LCH) 침범으로 나누며, MSLCH는 위험기관 침범 여부에 따라 위험기관 침범군(간, 비장, 조혈기관 중 적어도 하나 이상의 장기를 침범한 경우)과 위험기관 비침범군으로 다시 분류된다[ 8]. LCH의 확진을 위해서는 조직검사를 통한 병리학적 진단이 필요하다. LCH 세포는 hematoxylin-eosin 염색에서 균질하게 염색되는 분홍색 세포질을 가지며, 면역조직화학 염색에서 S-100 단백, CD1a 또는 langerin (CD207)에 양성인 세포를 확인하는 것이 필수적이다.
치료 방법에 있어서 단독적으로 피부 혹은 뼈 침범을 보이는 SS-LCH의 경우 국소요법이 권장되며, 국소요법 중 수술적 절제 방법은 SS-LCH 중에서도 단독 피부 병변에서 고려된다. 또한 피부에 발생한 SS-LCH 경우 methotrexate, 6-mercaptopurine 경구요법이 권장된다[ 11, 12]. 소아 환자와 달리 성인의 경우 뼈에 발생한 SS-LCH에서 허용 가능한 부작용에 한에서 방사선요법을 시행할 수 있다[ 13]. 이렇듯 SS-LCH에서의 치료는 피부와 뼈의 경우에서만 보고되어 있으며 다른 장기를 침범한 경우에 대해서는 거의 알려진 바가 없다. 두경부 영역에서는 후두에 발생한 SS-LCH가 6예 보고되었고, 치료로 방사선요법 및 외과적 절제가 시행되었다[ 14]. 또한 Eden 등[ 15]은 다양한 구강 부위에 발생한 LCH 13예를 보고 하였는데, 각 발생 부위를 보면 하악이 9예, 상악 3예, 잇몸 1예, 구개 2예, 볼 점막 1예, 혀 1예이다. 발생 부위에서 알 수 있듯이 23.1%에서만 뼈가 아닌 연조직에서 발생하였다. 절반에 가까운 환자(46.1%)에서 통증을 동반하지 않는 점차 커지는 종물로 병원을 내원하였고, 통증을 호소하는 경우가 15.4%, 무증상인 경우도 15.4%였다. 임상양상만을 보면 다양한 병변으로 오인될 수 있는데, 하악, 상악에 발생한 경우 뼈에 호발하는 호산구성육아종 또는 치근낭, 치성각화낭, 함치성낭과 같은 치아 관련 병변으로 오인될 수 있다. 13예 모두에서 수술을 통한 완전 절제를 시행하였고 저용량 방사선 요법을 진행하였다[ 15]. 본 증례와 같이 LCH가 혀나 구강 점막과 같은 연조직에 발생하는 경우 정상 점막으로 덮힌 종물의 형태로 신경초종, 신경섬유종, 평활근종 등과 감별이 필요하다. LCH는 병변의 명확한 경계 및 피막이 없이 주변 조직으로 침윤된 육아종성 조직 양상으로 MRI에서도 주변 조직과의 경계가 없는 침윤성 병변으로 보여진다. 진단을 위해서는 조직학적 확인이 가장 중요하겠으나 이러한 종물의 특징 및 영상의학적 특징을 통해 LCH를 임상적으로 감별하는 데 도움이 될 수 있겠다.
본 증례의 치료를 결정함에 있어서 단일계통 병변으로 항암치료와 같은 전신 치료보다는 국소치료를 진행하기로 결정하였고, 국소치료 중 외과적 절제의 경우 종물의 크기가 2 cm 이상으로 반절제술 범위의 혀가 절제될 가능성이 있었으며, 이로 인한 조음, 연하기능 저하가 발생할 가능성을 배제할 수 없었다. 결과적으로 저용량 방사선요법을 통해 병변의 성공적인 치료 효과를 확인하였다.
Notes
Author Contribution
Conceptualization: Geun-Jeon Kim. Writing—original draft: Geun-Jeon Kim, Hyun-Il Shin. Writing—review & editing: Sang- Yeon Kim, Dong-Il Sun.
Fig. 1.
Image of the tumor. The tumor was located on the left mid to lateral area of the intramucosal tongue. The size of the tumor was approximately 2 cm (boundary marked with blue arrows), initially (A). One-year post-radiotherapy follow-up visit demonstrated complete remission of the tongue mass (B). 
Fig. 2.
The MRI T1-weighted (A) and T2-weighted (B) sequence revealed a 1.8×1.4 cm-sized hyperintense mass in the left lateral tongue (indicated with yellow arrows). 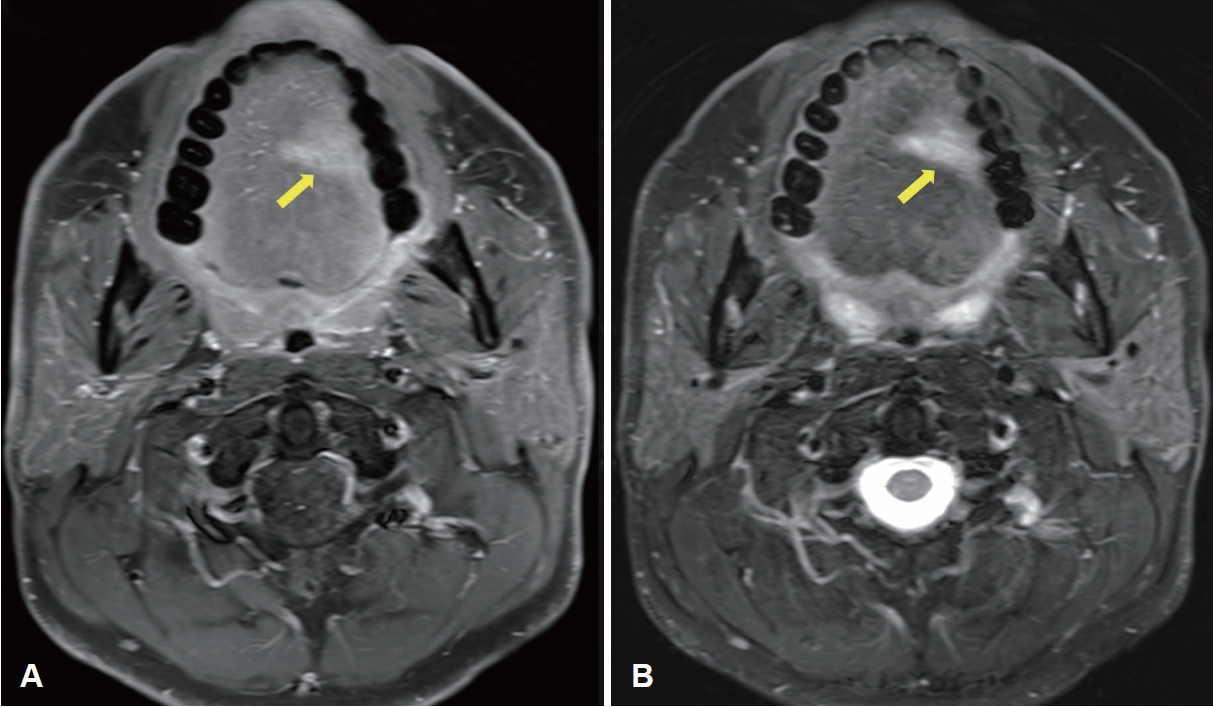
Fig. 3.
Results of pathological examination. The specimen contained patches of infiltrated histiocyte-like cells with lightly stained cytoplasm, some nuclear folding, and nuclear grooves. Multinucleated giant cells accumulated locally, admixed with eosinophils (hematoxylin- eosin staining, ×100) (A). The immunohistochemical staining results were CD1a (+) (×100) (B), S-100 (+) (×100) (C), and CD68 (+) (×100) (D). 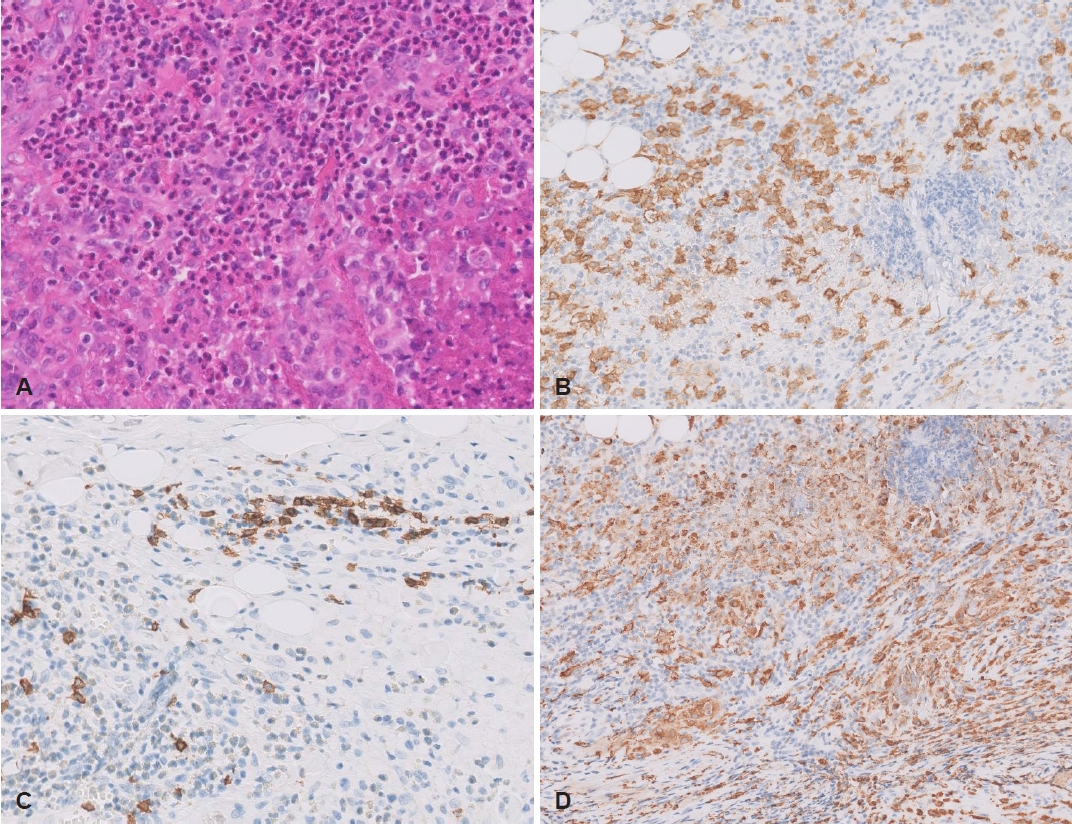
REFERENCES
1. Guyot-Goubin A, Donadieu J, Barkaoui M, Bellec S, Thomas C, Clavel J. Descriptive epidemiology of childhood Langerhans cell histiocytosis in France, 2000-2004. Pediatr Blood Cancer 2008;51(1):71-5.   2. Salotti JA, Nanduri V, Pearce MS, Parker L, Lynn R, Windebank KP. Incidence and clinical features of Langerhans cell histiocytosis in the UK and Ireland. Arch Dis Child 2009;94(5):376-80. 3. Arsovic N, Tomanovic N, Bukurov B. Sudden sensorineural hearing loss as first presenting symptom of unifocal Langerhans cell histiocytosis in the temporal bone. Otol Neurotol 2013;34(3):e24-5.
4. Krooks J, Minkov M, Weatherall AG. Langerhans cell histiocytosis in children: History, classification, pathobiology, clinical manifestations, and prognosis. J Am Acad Dermatol 2018;78(6):1035-44. 7. The French Langerhans’ Cell Histiocytosis Study Group. A multicentre retrospective survey of Langerhans’ cell histiocytosis: 348 cases observed between 1983 and 1993. Arch Dis Child 1996;75(1):17-24.  9. Weiss LM, Jaffe R, Facchetti F. Tumours derived from Langerhans cells. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, eds. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon: IARC; 2017. p. 470-2.
12. Steen AE, Steen KH, Bauer R, Bieber T. Successful treatment of cutaneous Langerhans cell histiocytosis with low-dose methotrexate. Br J Dermatol 2001;145(1):137-40. 13. Atalar B, Miller RC, Dincbas FO, Geismar JH, Micke O, Akyurek S, et al. Adult langerhans cell histiocytosis of bones: A rare cancer network study. Acta Orthop Belg 2010;76(5):663-8. 15. Eden P, Abeyasinghe WAMUL, Mufees MBM, Jayasooriya PR. A series of 13 new cases of langerhans cell histiocytosis of the oral cavity: A master of disguise. Oral Health Care 2017;2(1):1-4.
|
|














