Introduction
Ceruminous glands are modified apocrine glands located within the skin of the external auditory canal (EAC). Tumors arising from the ceruminous glands are rare, accounting for only 5.7% of all external ear tumors [1]. According to the World Health Organization, ceruminous gland tumors can be classified into six categories according to its histological characteristics; 1) ceruminous adenoma, 2) ceruminous pleomorphic adenoma, 3) ceruminous syringocystadenoma papilliferum (SCAP), 4) ceruminous adenocarcinoma, 5) adenoid cystic carcinoma, and 6) mucoepidermoid carcinoma [2].
SCAP was first mentioned as a “naevus syringadenomatosus papilliferus” by dermatologists in the 20th century [3]. SCAP occurs in the head and facial area in forms of infiltrative macules, papules, or keratinous nodules and also rarely occurs in the EAC, with 50% being found after birth and 15%-30% during childhood [4].
Less than 150 cases of SCAP have been reported up to date and even fewer of those arising from the EAC. In this report, we describe the surgical removal of SCAP originating from the EAC via retro-auricular approach in an adult patient.
Case
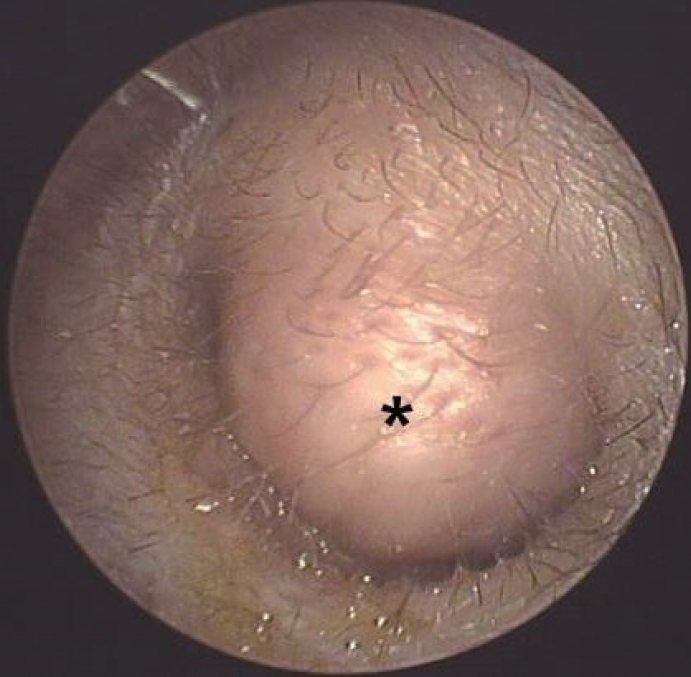
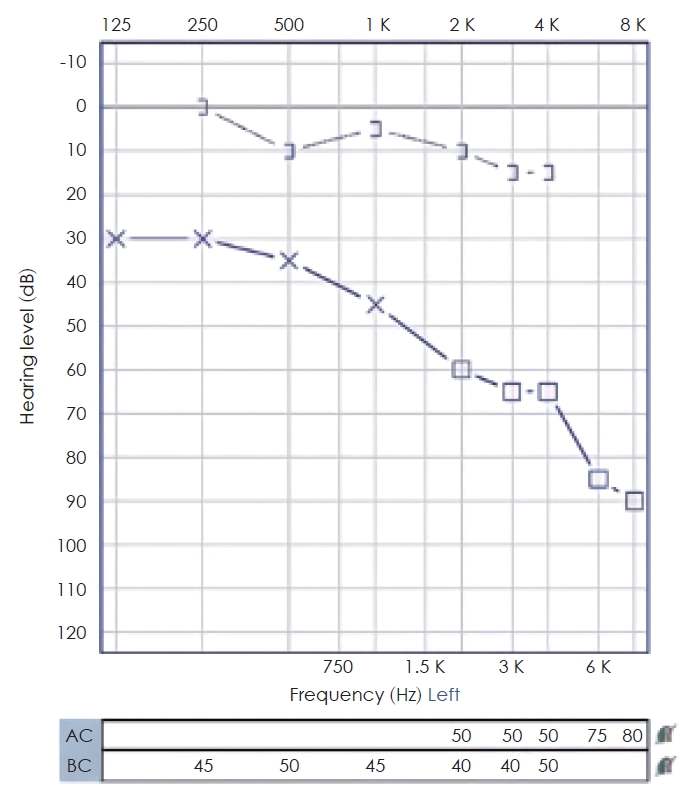
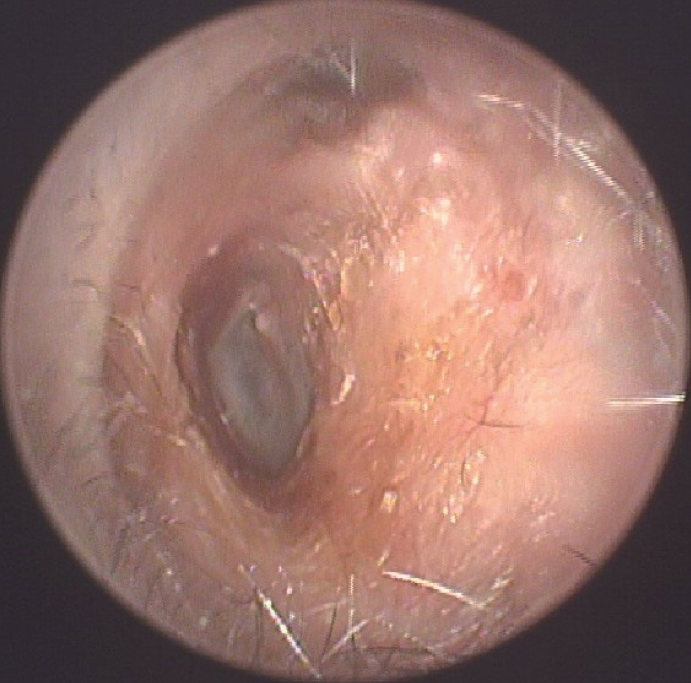
A 51-year-old male patient visited our hospital presenting with a left EAC mass found incidentally 2 years ago. He complained of left ear fullness and hearing loss. Otoscopy revealed a mass arising from the superior wall of the left EAC, completely obstructing the auditory canal. The mass had a diameter of approximately 1.5 cm and was soft to touch, having a clear boundary with yellow discharge surrounding it (Fig. 1). The tympanic membrane could not be seen due to the mass. Mixed type hearing loss up to 51 dB with an air-bone gap of 41 dB was identified in pure tone audiometry (Fig. 2).
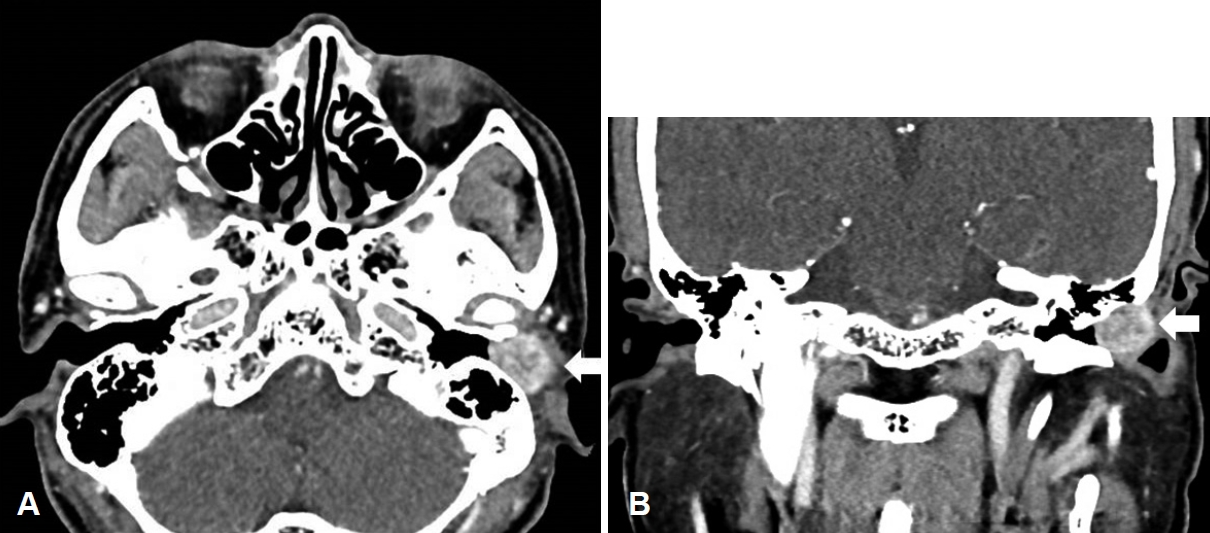
Enhanced temporal bone CT image confirmed an irregularly enhancing 1.7 cm sized round-shaped mass with clear margins located in the cartilaginous portion of the left EAC (Fig. 3A). Modification in the mastoid cortex due to the mass effect of the tumor was noted. Otherwise, there was no significant destruction of surrounding bony structures (Fig. 3B). Preoperative cranial nerve MRI with gadolinium enhancement showed a heterogeneous enhancing T1 low, T2 high lesion (Fig. 4).
The patient underwent microscopic surgery and the mass was resected via retro-auricular approach under general anesthesia. A 1.5×2×1 cm-sized elliptical mass with clear boundaries originating from the superior posterior portion of the EAC was confirmed and completely resected. The defect in the ear canal was reconstructed by elongation of the endomeatal skin followed by ear packing.
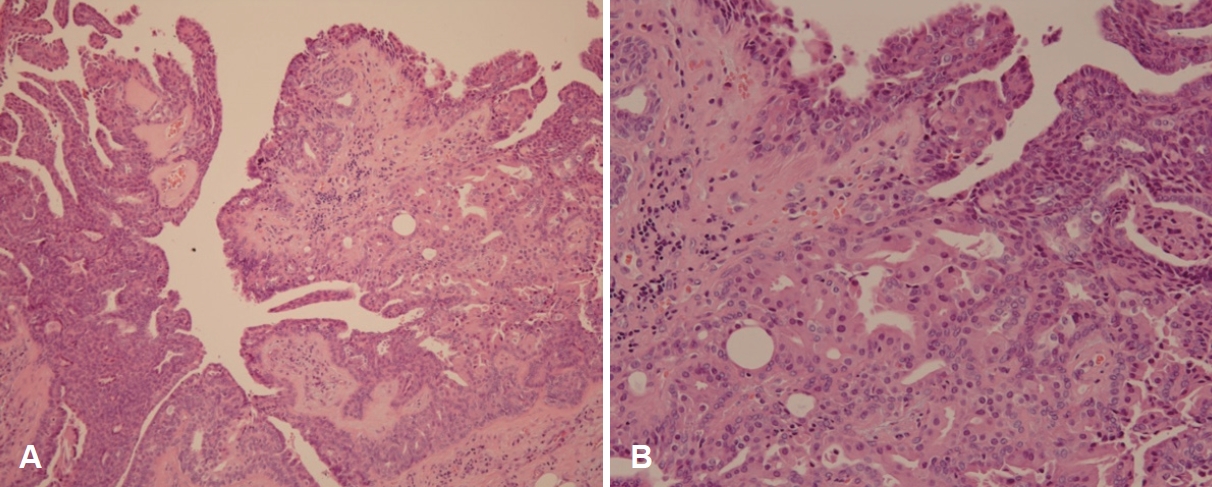
Histopathological examination confirmed the resected specimen as SCAP. The tumor showed dilated papillary and cystic structures (Fig. 5A) and was composed of luminal columnar epithelium with abundant eosinophilic cytoplasm and outer basal/myoepithelial cells (Fig. 5B).
The patient was discharged the day after the operation with no symptoms or complications. He visited the otorhinolaryngology outpatient clinic for regular follow ups and 4 months after the microscopic surgery, the resection site was well healed without any complications (Fig. 6).
This report was approved by the Institutional Review Board of the Bundang Jesaeng General Hospital (DMC 2022-03-008), and the requirement of informed consent was waived.
Discussion
SCAP is a benign adnexal tumor derived from the apocrine gland and is known to be associated with malignant tumors such as basal cell carcinoma, verrucous carcinoma, and tubular sweat gland carcinoma [5]. SCAP in the EAC may present with a range of symptoms depending on the degree of auricular canal blockage, from conductive hearing loss to aural fullness, otalgia, ear discharge and hemorrhage [6].
The characteristic pathological findings of SCAP are papillary hyperkeratotic epithelium with intradermal indentation. This papillary process connects directly with the tubular structure located deep in the indentation [7]. The process has a double layer within it, consisting of columnar epithelium abundant with eosinophilic cytoplasm and cuboidal epithelium with relatively scarce cytoplasm. Dense infiltration of plasma cells and lymphocytes are found in the interstitial space [8].
CT and MRI are important imaging modalities for the diagnosis of EAC tumors. While CT images show the location of the lesion and association with surrounding tissues, MRI images reveal the nature of the mass and help in differential diagnosis [8]. MRI of SCAP is reported to show intermediate signal intensity in both pre-contrast T1 and T2-weighted images, while showing weak enhancement in T1-weighted images with contrast. If the lesion shows low signal intensity in T2-weighted images or high enhancement after contrast, other types of tumors such as pleomorphic adenoma should be considered rather than SCAP [9].
Mammino and Vidmar [10] reported 144 cases of SCAP, of which 108 cases originated from the head and neck, 29 cases from the trunk, and 8 cases from the limbs. Since 11 cases of SCAP in the EAC reported by Müller and Theissig [11], 12 cases were reported up to date but the actual occurrence is considered to be more [12].
The low incidence and nonspecific symptoms of SCAP make the differential diagnosis of malignant neoplasms inevitable, also with the need for distinguishing benign ceruminous gland tumors, cholesteatoma, cholesteatomatous otitis media, and tuberculous otitis media [6]. In this case, we performed complete resection under general anesthesia as preoperative CT scans showed no evidence of infiltration into surrounding bone or tissue.
Complete tumor resection is the gold standard treatment for SCAP when there is no evidence of bony destruction in the surrounding EAC. Transcanal or retroauricular approach can be considered [6-8]. Although recurrence is rare following complete resection and current guidelines suggest no need for additional therapy, regular follow-up examination is recommended [6].
In conclusion we performed complete resection of the EAC tumor via retro-auricular approach under general anesthesia because preoperative CT scans showed no evidence of infiltration into the surrounding bone or tissue. SCAP was confirmed in histopathologic examination, and we report this case as SCAP in the EAC is an extremely rare case.