외이도에 발생한 동정맥기형 1예
Abstract
Benign vascular tumors are relatively common in the head and neck region, but are rarely found in the ear. Among vascular tumors, infantile hemangioma stands as the prevailing entity, characterized by a rapid initial proliferation of endothelial cells, succeeded by a gradual regression over the course of several years. In contrast, arteriovenous malformation (AVM) is a less common phenomenon, originating from peripheral vascular anomalies during embryogenesis, and it does not undergo spontaneous regression. Specifically, the occurrence of AVM within the external auditory canal are exceedingly uncommon. Here, we describe a case of a 49-year-old male patient who had a mass incidentally discovered in the external auditory canal, but refused initial treatment. He later returned as the mass enlarged. This case could have been clinically misdiagnosed as a hemangioma, but was ultimately diagnosed pathologically as an AVM.
Key words: Arteriovenous malformation ㆍ Ear canal ㆍ Vascular tissue neoplasm
서 론
양성 혈관성 종양(benign vascular tumor)은 두경부 부위에 비교적 흔하게 발생하지만 귀에서 발견되는 경우는 적으며 특히 외이도 내에 국한되어 위치한 경우는 극히 드물다. 외이도에서 발견되는 혈관 기형은 대부분 혈관종(hemangioma)이며 국내에서도 보고된 4예를 포함하여[ 1- 4] 현재까지 세계적으로 20예 정도가 보고된 바 있다. 반면 동정맥 기형(arteriovenous malformation)은 혈관종보다 드물게 나타나며, 전신 어디에나 생길 수 있으나 외이도 내에서 발견된 경우는 세계적으로 1예만 보고되었고 국내에서는 아직까지 보고된 바 없다[ 5]. 저자들은 이충만감을 주소로 발견된 외이도에 국한된 혈관성 병변을 일괴 적출한 외이도 동정맥 기형 1예를 경험하였기에 이를 문헌고찰과 함께 혈관종과의 차이를 비교하여 보고하고자 한다.
증 례
49세 남자가 10년 전부터 지속된 좌측 이충만감으로 내원하였다. 9년 전 동일 증상으로 본원 내원 후 좌측 외이도 후방의 푸른 종물이 발견되었으나 추적 소실되었던 환자로 최근 증상이 악화되어 내원하였다. 과거력상 특이 병력이 없는 환자로 시행한 이내시경상 좌측 외이도 후방에서 기원하여 외이도를 가득 채우고 있는 박동성이 없는 푸른색을 띈 창백한 종물이 발견되었으며 고막은 종물로 인해 확인할 수 없었다( Fig. 1A). 순음청력검사상 좌측 귀의 고주파에서 10 dB 이내의 골도-기도차를 보였으나 청력은 우측 6 dBHL, 좌측 8 dBHL로 정상이었다( Fig. 1B). 측두골 전산화단층촬영상 좌측 외이도의 골부 초반부를 가득 채우고 있는 조영증강이 되는 종양이 관찰되었으며 주변으로 미세한 골 미란을 동반하고 있었다( Fig. 1C and D). 최근 환자의 증상이 악화되었으며 9년 전보다 종물 크기가 증가한 소견이 있어 혈관성 종양을 의심하여 수술적 적출을 계획하였다. 완전 절제를 위하여 전신마취하 후이개 접근법을 통해 좌측 외이도 후방의 피부 피판을 들어올려 종물에 접근하였다( Fig. 2A). 혈관성 종물은 외이도 골부에서 쉽게 박리되었고 외이도 피부의 일부와 함께 일괴 적출하였다( Fig. 2B). 종물 제거 후 외이도 후방 골부에서 유양동 쪽으로의 혈관 천공 분지와 이에 따른 골공(bony hole)을 관찰할 수 있었다. 이는 술전 측두골 컴퓨터단층촬영에서 관찰된 미세한 골 미란이 혈관 천공 분지가 지나가는 부위임을 짐작해 볼 수 있었다. 이후 드릴로 외이도 벽을 매끄럽게 해준 후( Fig. 2C) 혈관 천공 분지로 인한 골공을 TachoSil (Hyundai Pharm, Seoul, Korea)과 연골로 보강하였고( Fig. 2D) 측두골 골막을 이용하여 외이도 후벽 피부를 재건하였다( Fig. 2E). 제거한 종물은 1.2×0.4×0.3 cm 크기로 병리조직학적으로 다양한 크기의 확장된 혈관들로 구성되어 있었으며( Fig. 3A), 혈관벽은 한 겹의 flat한 세포들로 이루어졌으며 세포에서 mitotic activity는 관찰되지 않았다( Fig. 3B). 섬유내막 비후로 인한 다양한 두께의 벽 증식을 동반하고 있었으며( Fig. 3C), 동맥화된 정맥의 탄성판이 잘 확인되어 동정맥 기형으로 진단되었다( Fig. 3D and E). 수술 당일 합병증 없음을 확인 후 퇴원하였고 술후 7일째 외이도 팩킹을 제거하였고 3주째 이내시경으로 확인한 결과 외이도 안정적이며 정상 고막 확인되었다( Fig. 2F). 술후 2달 동안 재발의 징후 및 합병증 없었으며 외래 추적관찰 중이다.
고 찰
1982년 Mulliken과 Glowacki [ 6]는 과거 “혈관종(hemangioma)”라고 통칭되어 불리던 혈관성 병변을 크게 혈관성 종양(haemangiomata, vascular tumor)과 혈관 기형(vascular malformation)으로 분류하였고 이후 International Society for the Study of Vascular Anomalies에서 이를 기반으로 혈관성 병변에 대한 세분화된 분류를 제시하였다[ 7]. 혈관종은 두경부 영역에서 흔히 발견되며 혈관 내피 세포의 증식을 특징으로 하며 병리조직학적 소견에 따라 해면상, 모세상, 혼합종으로 나뉜다. 이는 가장 흔한 영유아기 선천성 종양이며 12세까지는 대부분 자연 관해되는 것으로 알려져 있으며, 외이도 종물로 발견된 경우는 드물며 발견된 경우의 대부분이 해면상 혈관종으로 보고되고 있다[ 3]. 이에 반해 동정맥기형은 혈관 내피 세포의 증식 없이 나타나는 혈관 구조의 이상이며 혈관종과 달리 자연관해 되지 않으며 나이가 듦에 따라 크기가 커지는 경향이 있다. 조직학적으로 증가된 혈류로 인해 비후된 두꺼운 벽을 가진 동맥과 정맥의 소견을 보이며 크기의 증가는 세포의 증가보다는 증가된 혈류에서 기인하는 것으로 보인다[ 5]. 2004년 후이개동맥(posterior auricular artery)에서 기원한 외이도의 동정맥기형이 처음 보고된 바 있다[ 8]. 증상은 무증상부터 환측의 청력저하, 이충만감, 이명, 이통, 이루 등 다양하게 나타나며 본 증례의 경우 초기에는 증상이 심하지 않았으나 종물의 크기가 증가함에 따라 이충만감과 경도의 전음성 난청을 동반하였을 것으로 생각된다. 이학적 검사상 외이도와 고막에서 표면이 매끄럽고 모양이 둥근 종물로 관찰되며 측두골 전산화단층촬영상에서 관찰되는 외이도의 비정상적인 연부조직 음영이 특징적인 소견이다[ 9]. 본 증례에서도 측두골 전산화단층촬영에서 조영증강되는 연조직 음영의 종물이 외이도 후벽에서 관찰되었으며 혈관으로 인한 골공으로 생각되는 미세한 골미란 소견은 보였으나 골침범이나 중이로의 침범은 없는 것을 확인할 수 있었다. 자기공명영상촬영, 혈관 조영술도 진단에 사용할 수 있으나 대개 시행하지 않으며 혈관종, 화농성 육아종, 고실사구종양, 고위경정맥구, 흑색종 등과의 감별 진단이 필요하다[ 4]. 외이도 동정맥 기형은 크기가 작거나 증상이 없을 경우 치료가 필요치 않으며 증상이 있는 경우 완전한 수술적 절제를 고려해야 한다. 수술 시에는 외이도의 피부를 보존하는 것이 중요하며 혈관 천공 분지와 그에 의한 골공이 관찰될 수 있기 때문에 수술 전 초선택적 혈관 조영술을 통한 색전술(superselective embolization)을 시행해볼 수 있으며 수술 중에도 혈관 천공 분지에 대한 처치를 고려하여 시행해야 한다[ 8, 10]. 동정맥 기형의 크기가 크거나 피부 보존이 어려울 경우, 환자가 수술을 원치 않을 경우 색전술이나 경화치료를 우선적으로 고려해볼 수도 있다. 하지만 수술 없이 색전술 단독을 시행하거나 종물을 일부 절제하는 것은 새로운 측부 혈관(collateral vessel)을 만들고 크기를 증가시켜 병변을 악화시킬 수 있기 때문에 지양해야 한다[ 5]. 또한 경화 치료 시 국소적인 괴사나 피부 궤양, 누공 등이 발생할 수 있기 때문에 시술 후 경과 관찰이 중요하며 이러한 합병증이 발생한 경우 2차적 수술을 통한 수술적 절제 및 피부 피판술을 고려해야 한다[ 11].
ACKNOWLEDGMENTS
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HR22C1302). This work was supported by Korea University Research Fund (K2306671, K2310471, K2306031, K2208471, K2205081, K2125741, K2211761).
Notes
Author Contribution
Conceptualization: Gi Jung Im. Validation: Gi Jung Im, Soo Jeong Choi. Funding acquisition: Gi Jung Im. Writing—original draft: Gi Jung Im, Soo Jeong Choi. Writing—review & editing: all authors.
Fig. 1.
Preoperative evaluation. A: Endoscopic findings in left external auditory canal. A pale blue mass (arrow) was observed on the left posterior wall and it was filling the left external auditory canal. B: Pure tone audiometry was normal on both side, but slight air-bone gap was observed on the left ear. Enhanced temporal bone CT scan. C and D: Axial view (C) and coronal view (D). A contrast-enhanced mass was located on the initial bony part of the left posterior external auditory canal, accompanied with slight bony erosion (arrow). 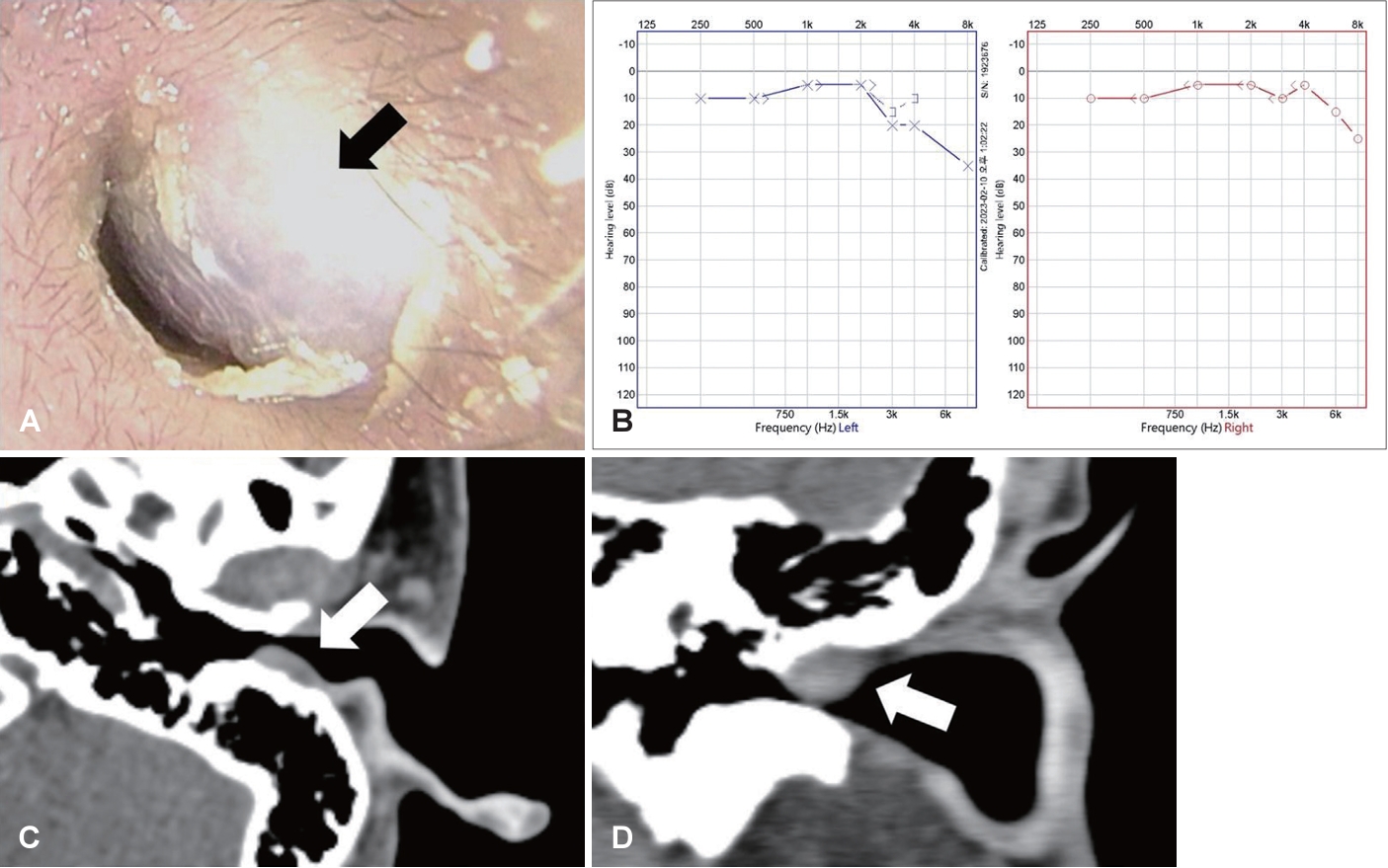
Fig. 2.
Perioperative image. A: Posterior auricular approach was done. The skin flap on the posterior external auditory canal was elevated to access the mass (arrow). B: Vascular mass (arrow) was seen and en-bloc resection was done including the nearby skin. The mass was easily removed from the mastoid bone. C: After removing the mass, a perforating vessels and bony hole was observed in the posterior bony part of the external auditory canal. Smoothing the bony canal was done with diamond drill (arrow). D: The bony hole by the perforating vessels was reinforced with TachoSil (Hyundai Pharm) and cartilage (arrow). E: The skin of posterior external auditory canal was reconstructed by using the temporal bone periosteum (arrow). F: After 3 weeks later, the external auditory canal was stable (arrow) and normal tympanic membrane was seen. 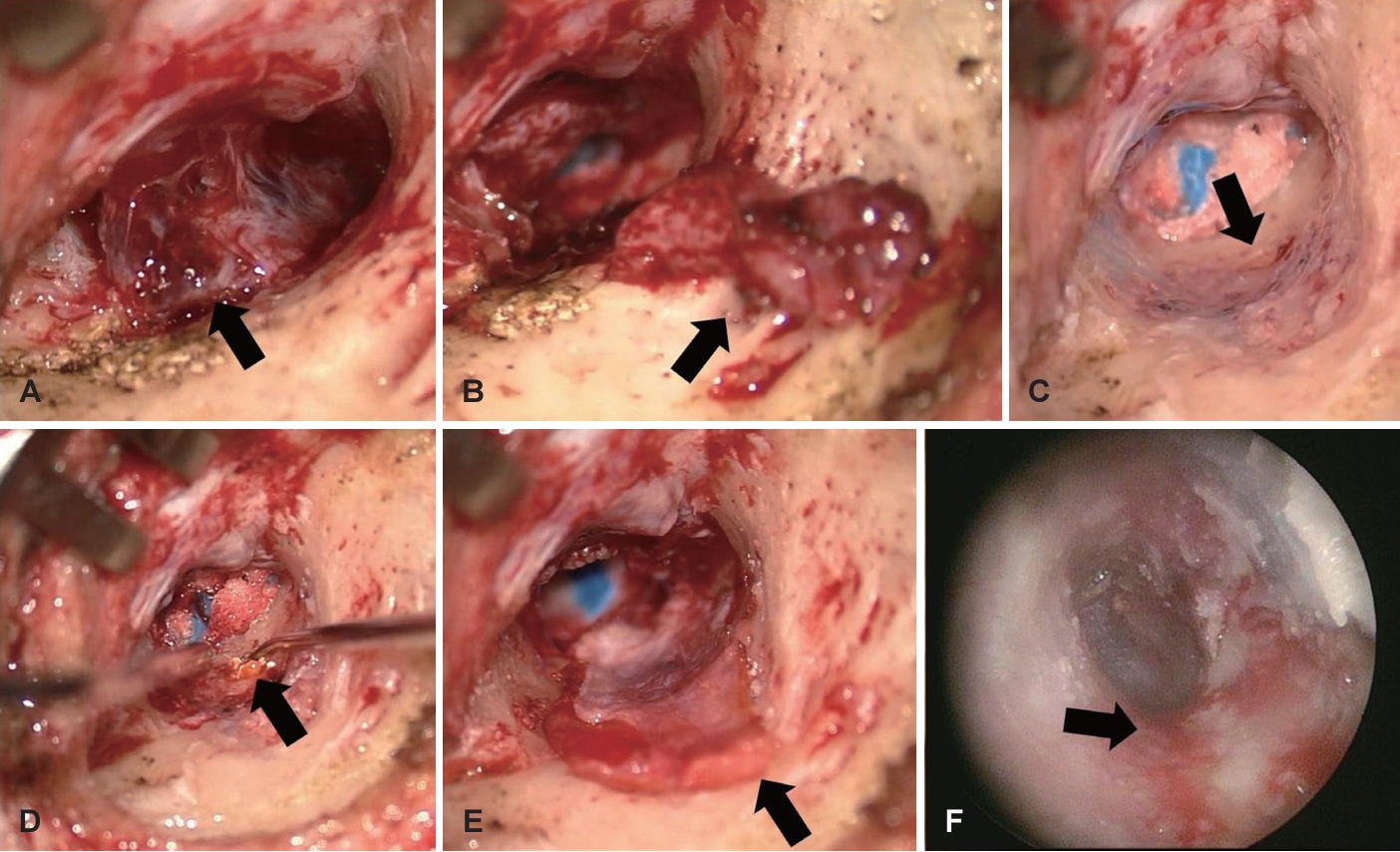
Fig. 3.
Representative microscopic images. A: Arteriovenous malformation composed of irregular dilated vasculatures (arrows, hematoxylin and eosin [H&E], ×12.5). B: Flat monolayered endothelial lining without mitotic activity (arrows, H&E, ×100). C: Fibrointimal thickening (arrows, H&E, ×100) D: Arterialized vein with variable mural thickening (arrows, H&E, ×100) E: Elastic lamina in arterialized vein (arrows, elastic stain, ×100). 
REFERENCES
1. Cho KH, Kim KH, Lee KS, Yang HS. A case of capillary hemangioma in the exter nal auditor y canal. Korean J Otorhinolaryngol-Head Neck Surg 2001;44(9):993-6.
2. Kim H, Seo J, Lee HJ. A case of hemangioma in the external auditory canal with pulsatile tinnitus. Korean J Otorhinolaryngol-Head Neck Surg 2017;60(3):140-3.   3. Kim YJ, Kwon AY, Kim HM. A case of benign vascular tumor of tympanic membrane. Korean J Otorhinolaryngol-Head Neck Surg 2015;58(4):290-3. 4. Song SY, Choi YH, Bai CH. Cavernous hemangioma of the external auditory canal: a case report. Korean J Otorhinolaryngol-Head Neck Surg 2006;49(8):845-8.
5. Kim SH, Han SH, Song Y, Park CS, Song JJ. Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature. Braz J Otorhinolaryngol 2017;83(6):683-90.  6. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 1982;69(3):412-22. 8. Raghu M, De R, Higgins N, Axon P. Spontaneous arteriovenous malformation of the external auditory meatus. J Laryngol Otol 2004;118(11):912-3. 9. Chakeres DW, Kapila A, LaMasters D. Soft-tissue abnormalities of the external auditory canal: subject review of CT findings. Radiology 1985;156(1):105-9. 11. Sannier K, Dompmartin A, Théron J, Labbé D, Barrellier MT, Leroyer R, et al. A new sclerosing agent in the treatment of venous malformations: study on 23 cases. Interv Neuroradiol 2004;10(2):113-27.
|
|














