Introduction
Benign sinonasal tumors are clinically and histopathologically diverse and often present with similar clinical symptoms. Common symptoms include nasal obstruction, epistaxis, anosmia, and rhinorrhea [1]. They may also be asymptomatic or incidentally detected during imaging studies performed for other reasons.
Inverted papilloma (IP) and angiofibroma are benign sinonasal tumors. IP occurs at a rate of 0.2 to 6 cases per 100000 patients per year and accounts for 0.5% to 4.0% of sinonasal tumors. Angiofibroma is even rarer, with an incidence of approximately 1 in 150000 [1]. Both tumors typically exhibit a more vascular appearance than typical nasal polyps during endoscopic examinations and present with nonspecific clinical symptoms. Therefore, accurate diagnosis is crucial for differentiating between them and selecting appropriate treatment strategies.
Herein, we present an exceptionally rare case of concurrent IP and angiofibroma in the nasal cavity. By sharing this case, we would underscore the importance of precise diagnosis and surgical management and highlight that IP and angiofibroma can coexist within the nasal cavity.
Case
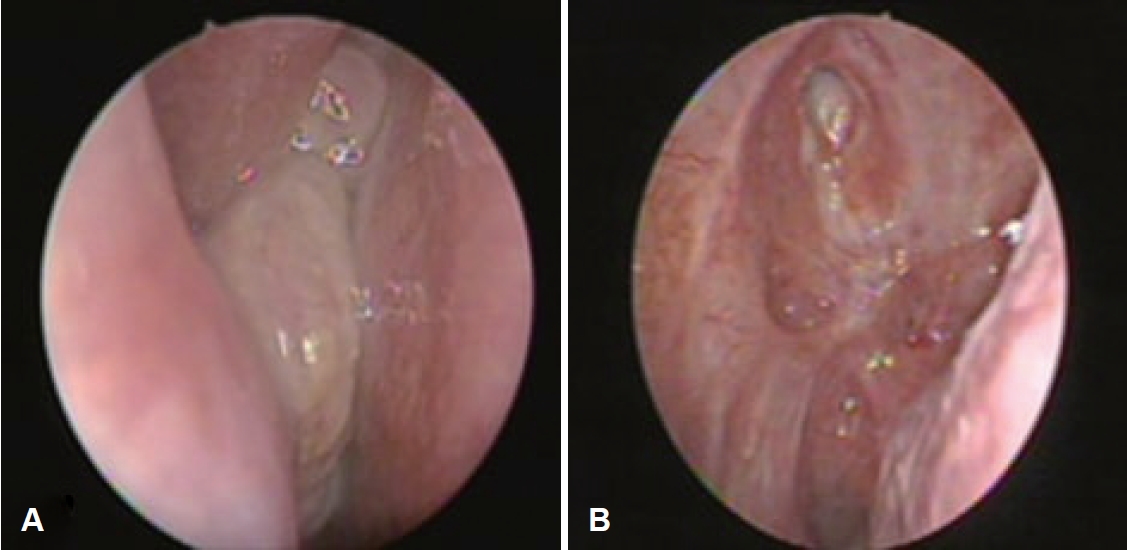
A 77-year-old female presented with a mass in the right nasal cavity which was incidentally discovered on brain CT and MRI taken after a traffic accident. The patient did not report any nasal symptoms such as obstruction or epistaxis and had no underlying conditions other than hypertension. Endoscopic examination revealed a polypoidal, solid, and whitish mass in the right nasal cavity (Fig. 1A). A punch biopsy of the right nasal cavity mass performed at an outpatient clinic revealed benign hyperplastic squamous epithelium consistent with IP.
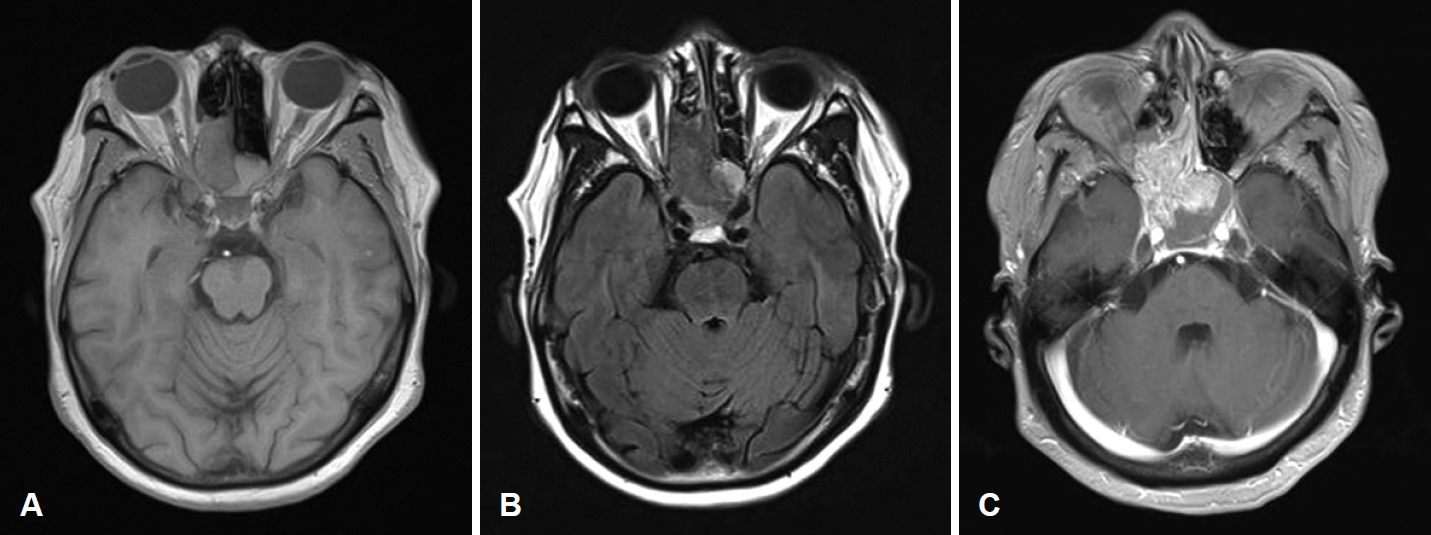
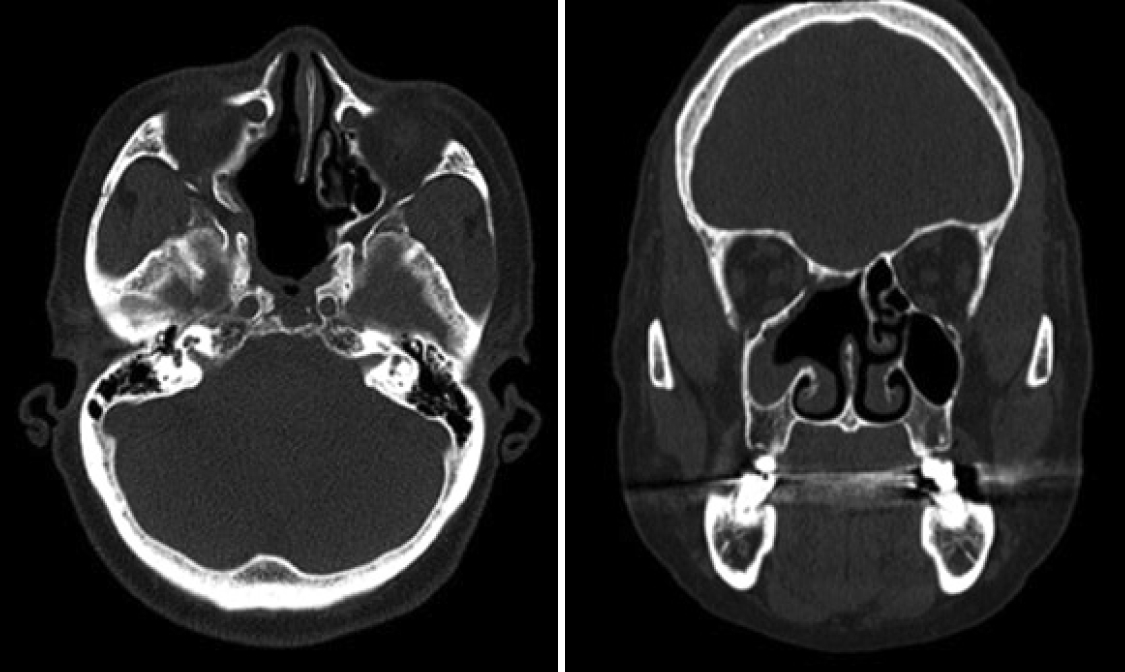
MRI scan findings were consistent with an intermediate signal on T1-weighted image (Fig. 2A), and heterogenous signal which includes presence of flow voids on T2-weighted image (Fig. 2B). Heterogenous enhancement was shown on contrast-enhanced T1-weighted image (Fig. 2C). Enhanced facial CT showed a 4 cm enhancing solid mass involving the right posterior nasal cavity, extending into the right ethmoid sinus and right sphenoid sinus, with evidence of bony erosion (Fig. 3). The left sphenoid sinus exhibited a non-enhancing mucoid density suggestive of sinusitis. Based on the imaging findings, the lesion was more consistent with an angiofibroma. Surgical treatment was decided accordingly.
One day before surgery, preoperative angiography was performed and in the process of selecting internal maxillary artery through right external carotid, hypervascular staining was observed in the right nasal cavity on angiogram, so the feeding vessel of tumor was thought to be internal maxillary artery (Fig. 4A). Embolization was successfully performed by using gelfoam, and a follow-up angiogram showed resolution of the hypervascular staining (Fig. 4B).
Subsequently, endoscopic sinus surgery and endoscopic tumor removal was performed. Operators used the BiZact device during tumor removal to minimize blood loss during surgery, and the tumor was removed piecemeal. The origin of the IP was identified to be a sphenopalatine area, and IP occupied the natural opening of the right maxillary sinus, between the septum and right middle turbinate, and in the right ethmoid sinus and the inferior-anterior and posterior walls of the right sphenoid sinus.
The final biopsy results of the mass indicated the co-existence of IP and angiofibroma. The lesion showed features of a sinonasal papilloma with inverted growth pattern (Fig. 5A), along with vascular spaces of various sizes, ranging from dilated branching vessels to slit-like capillaries filled with fibrinous thrombi and an edematous to collagenous stroma, characteristic of angiofibroma (Fig. 5B).
Discussion
IP is a benign sinonasal epithelial tumor that is distinguished from other sinonasal tumors by based on three main characteristics: relative local aggression, high recurrence rates, and potential for malignancy [2]. Clinical examination via endoscopic exploration of the nasal cavity typically reveals a reddish-grey lobulated tumor. The tumor is firmer than an inflammatory polyp and has a characteristic вҖңraspberryвҖқ appearance [3]. Angiofibroma is another benign tumor unique to the sinonasal tract. It is a locally invasive vasoformative neoplasm that occurs almost exclusively in adolescent males [4]. Angiofibroma is commonly thought to be rare in elderly [5]; however patient in our case was 77-year-old female. Angiofibroma is hypothesized to be a testosterone-dependent tumor, and estrogen is known to affect in decreasing in the size of tumor [6]. Considering the patientвҖҷs age, occurrence of angiofibroma after menopause which leads to reduction of estrogen may support this rare case.
Most accepted theory of IP occurrence is that it arises from the metaplasia of respiratory epithelium into a squamous type, triggered by factors like chronic inflammation, exposure to irritants including smoking and occupational pollutants, or viral infections such as human papillomavirus (HPV) [7]. Recent documentation suggests a potential association between HPV infection and angiofibroma. A small study found a strong association between angiofibroma and HPV, detecting HPV-specific proteins and DNA within nasopharyngeal angiofibroma tissue, with no corresponding infection in the control groupвҖҷs adenoidal tissue [8]. Considering the increase in HPV incidence, the authors of this case speculated that the simultaneous occurrence of IP and angiofibroma in this case may be due to HPV infection.
To our knowledge, till date only one reported case of the coexistence of IP and angiofibroma in the nasal cavity [9]. According to this report, IP was suggested in a punch biopsy, and non-enhanced facial CT showed heterogeneous soft tissue density in the left maxillary sinus and nasal cavity with no extension to the nasopharynx. Open partial maxillectomy was performed to completely excise the tumor; however, significant bleeding occurred during the operation, which was difficult to control. The difference in our case is that a preoperative enhanced facial CT was taken, allowing for the consideration of angiofibroma and the possibility of performing an embolization procedure. Because angiofibroma has a high tendency to bleed, sometimes disastrously, an accurate and definitive preoperative diagnosis is necessary to prevent complications during surgery and pre-operative embolization has become the main treatment modality for angiofibroma [10].
In a similar paper about IP mistaken for angiofibroma in 19-year-old adolescent male, authors considered the mass to be an angiofibroma considering the patientвҖҷs age and enhancement found in facial CT, and preoperative embolization and subsequent transnasal endoscopic tumor excision was performed [11]. However, IP has been confirmed in permanent biopsy and the patient had a recurrence. As seen in this report which shows atypical clinical presentation, it becomes difficult to detect the disorder correctly, and the risk of recurrence rises due to inadequate diagnosis and treatment.
As the symptoms of these tumors are similar, the diagnosis of sinonasal tumors relies almost entirely on the histopathological results of a punch biopsy before treatment. However, it is crucial not to rely solely on biopsy results. The findings from imaging tools must be considered simultaneously. In particular, CT shows different patterns of bone erosion. Angiofibroma spreads have three patterns of bony involvement: 1) bone remodeling by means of expansion, thinning, and displacement; 2) cancellous bone invasion; and 3) bone resorption and destruction [12]. Otherwise, IP shows changes in bone including intratumoral calcification, thinning, bowing, erosion, and sclerosis in CT [13].
Due to its extremely low incidence rate and similar presenting clinical symptoms, otolaryngologists can overlook the occurrence of both angiofibroma and IP in the nasal cavity. In our case, discrepancies between the punch biopsy and the enhanced facial CT scan. Punch biopsy suggested a benign hyperplastic squamous epithelium, indicating IP, whereas facial CT revealed a 4 cm enhancing mass with features of angiofibroma. Not ignoring this difference in which each cannot occur when each tumor occurs alone, appropriate process such as embolization could be performed before surgery. While understanding the typical clinical features of each tumor, when there is an atypical aspect, clinicians should be aware of the possibility of simultaneous occurrence without ignoring it. It will eventually lead to an accurate treatment and prevention of recurrence.
This study was conducted with a deliberation exemption (IRB No. 2023-12-015) by the Institutional Review Board of the Kosin University Gospel Hospital.