Advanced Neuroendocrine Carcinoma of the Pharyngolaryngeal Region With Distant Metastasis: A Report of Two Cases
원격전이를 동반한 인후두 영역의 진행성 신경내분비암종 2예
Article information

Abstract
Neuroendocrine carcinoma (NEC) of the head and neck is a rare and aggressive malignancy accounting for less than 1% of head and neck cancers. Its nonspecific presentation mimics squamous cell carcinoma, and immunohistochemistry is essential for diagnosis. We report two cases of NEC arising in the pharyngolaryngeal region. The first patient, a 50-year-old male, presented with oropharyngeal NEC with mixed small and large cell features and synchronous hepatic and pulmonary metastases; he was treated with palliative chemotherapy. The second, a 64-year-old male, had small cell NEC of the left aryepiglottic fold with a pulmonary nodule; he underwent CO2 laser-assisted supraglottic partial laryngectomy and pulmonary wedge resection, followed by chemotherapy and radiotherapy. Both cases were confirmed by synaptophysin and CD56 positivity. These cases underscore the need for accurate immunohistochemical diagnosis, comprehensive staging, and multidisciplinary treatment.
Introduction
Neuroendocrine tumors of the head and neck, formerly termed carcinoid tumors, are rare neoplasms accounting for less than 1% of all head and neck malignancies [1,2]. The 2022 World Health Organization (WHO) classification, aligned with the International Agency for Research on Cancer framework, established a unified nomenclature [3].
Under this classification, epithelial neuroendocrine neoplasms (NENs) are divided into well-differentiated neuroendocrine tumors (NETs; graded G1-G3) and neuroendocrine carcinomas (NECs), the latter subtyped into small cell and large cell variants (Table 1). NECs are characterized by >10 mitoses/2 mm2 and Ki-67 >20% [3].
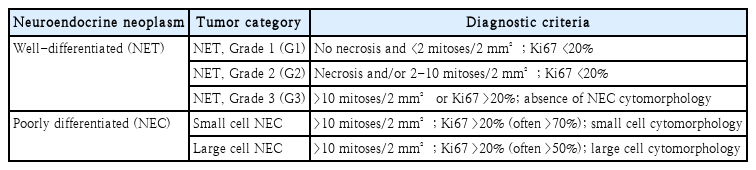
The 2022 WHO classification of epithelial neuroendocrine neoplasms of the upper aerodigestive tract and salivary glands
Diagnosis is challenging because NEC is clinically indistinguishable from squamous cell carcinoma (SCC); immunohistochemistry with synaptophysin, chromogranin A, and CD56 is essential [3,4]. NECs exhibit aggressive behavior with early metastasis and 5-year survival of 13%-46% [5,6]. A meta-analysis of 436 laryngeal NECs favored chemoradiotherapy over surgery alone, and the 2024 European Society for Medical Oncology (ESMO) guideline recommends multimodal therapy [7,8]. Standardized guidelines specific to head and neck NEC remain lacking. Herein, we report two cases of NEC arising in the head and neck region.
Cases
Case 1
A 50-year-old male with a 30-pack-year smoking history, hyperthyroidism, and hypertension presented with a 5-month history of globus sensation, bilateral nasal obstruction, and foul odor. No cervical mass was noted initially. Flexible endoscopy revealed an extensive ulceroinfiltrative mass involving the soft palate, bilateral palatine tonsils, uvula, epiglottis, pre-epiglottic space, and left aryepiglottic fold (Fig. 1).
Clinical presentation of Case 1. A: Oropharyngoscopic examination reveals a mass involving the soft palate and uvula. B: Laryngoscopic view demonstrates tumor extension into the epiglottis, aryepiglottic fold, and hypopharynx.
Uvular punch biopsy revealed nests and rosette-like glandular structures of mixed large and small tumor cells with geographic necrosis and brisk mitoses (Fig. 2). Immunohistochemistry showed diffuse positivity for cytokeratin 7, CD56, and synaptophysin, while chromogranin A and p16 showed focal positive staining. TTF-1, C-kit, p40, and S-100 protein stains were negative. Ki-67 reached 80%. The tumor was diagnosed as NEC with mixed small and large cell features.
Histopathology of Case 1. Uvular punch biopsy showing characteristic morphologic features of NEC, including diffusely distributed rosette-like glandular structures, a representative example of which is circled (A: hematoxylin and eosin [H&E] ×200), and diffuse positive immunohistochemical staining for synaptophysin (B: immunohistochemistry ×200). NEC, neuroendocrine carcinoma.
Contrast-enhanced neck MRI showed multilevel cervical and retropharyngeal lymphadenopathy (Fig. 3). Whole-body FDG PET-CT revealed hypermetabolic uptake at the primary and bilateral cervical nodes (Fig. 4), a 7.5 cm hepatic mass, and multiple pulmonary nodules (Fig. 5). Ultrasound-guided biopsies of a left level Ib node and the hepatic mass showed histopathology identical to the uvular lesion.
Contrast-enhanced neck MRI of Case 1. A: Axial T1-weighted image at the oropharyngeal level showing an extensive mass involving the soft palate and bilateral palatine tonsils (arrow). B: Axial T1-weighted image at the hypopharyngeal level demonstrating tumor extension to the epiglottis and left aryepiglottic fold (arrow). C: Sagittal T1-weighted image showing the full craniocaudal extent of the lesion spanning both levels (arrows).
FDG PET-CT of Case 1 (neck). A: Axial image showing hypermetabolic uptake at the primary oropharyngeal lesion (central arrow) and bilateral cervical lymph nodes (lateral arrows). B: Axial images at different levels, both demonstrating hypermetabolic uptake at the primary oropharyngeal lesion (arrows).
Whole-body FDG PET-CT of Case 1 (maximum intensity projection). Arrows indicate the hypermetabolic oropharyngeal primary lesion with adjacent cervical lymph node metastases, multiple pulmonary metastases, and hepatic metastasis, consistent with widespread metastatic disease.
Given multifocal regional and distant metastases, palliative carboplatin-etoposide was initiated. After eight cycles, progressive disease prompted a switch to second-line FOLFIRI. The patient subsequently received palliative radiotherapy to the oropharynx concurrent with second-line chemotherapy for pain control, and is currently receiving third-line topotecan therapy. The detailed treatment course and response evaluation over an 11-month follow-up period are summarized in Table 2.
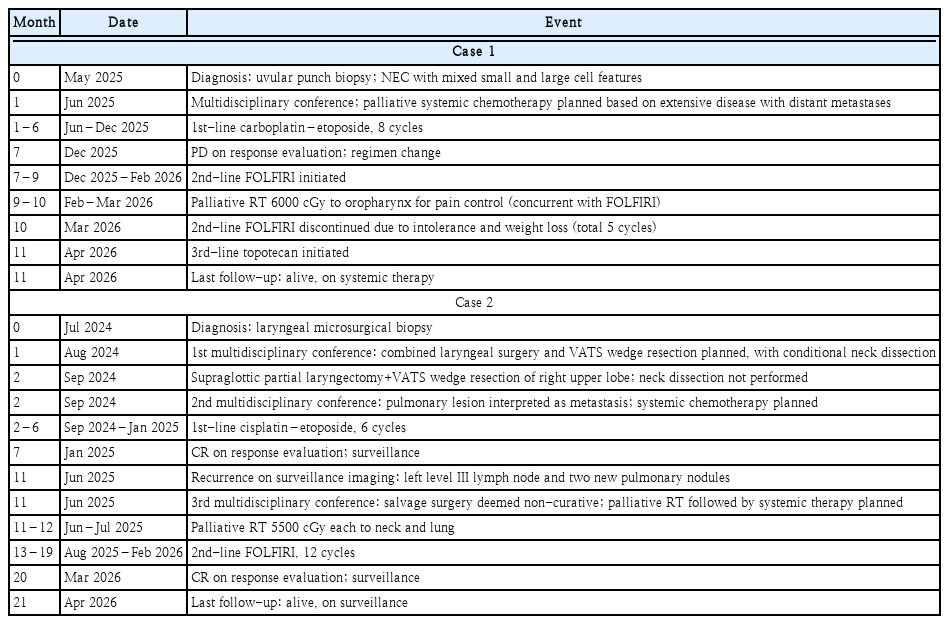
Chronological treatment course and response evaluation of both cases
Case 2
A 64-year-old male (40-pack-year smoker) presented with a 3-month history of progressive throat discomfort and odynophagia. He had undergone laryngeal microsurgical biopsy at a prior institution. At our institution, laryngoscopy confirmed a 2.4 cm mass at the left aryepiglottic fold without vocal fold fixation (Fig. 6A).
Endoscopic findings of Case 2. A: Preoperative view showing a mass at the left aryepiglottic fold. B: Postoperative 6 months demonstrating complete mucosal epithelialization.
The laryngeal microsurgical biopsy from the referring institution revealed a carcinoma suggestive of NEC. Immunohistochemistry showed positivity for p16, CD56, and synaptophysin, with focal p63 expression. Chromogranin A was negative, and the Ki-67 index was approximately 40%-50%.
Neck MRI showed a well-circumscribed lesion at the left aryepiglottic fold without adjacent invasion, and a 1.6 cm left level III lymph node without extranodal extension (Fig. 7). FDG PET-CT confirmed hypermetabolic uptake at both sites and identified a 1.2 cm hypermetabolic nodule in the right upper lobe (Fig. 8). Fine needle aspiration of the cervical node revealed metastatic carcinoma.
Contrast-enhanced neck MRI of Case 2. (A) Axial and (B) coronal T1-weighted images showing a well-circumscribed lesion at the left aryepiglottic fold and left level III cervical lymphadenopathy (arrows).
FDG PET-CT of Case 2. A: Axial image of the neck showing increased FDG uptake at the primary tumor and ipsilateral level III lymph node. B: Axial image of the chest revealing a hypermetabolic nodule in the right upper lobe (arrow).
Following multidisciplinary discussion, the pulmonary nodule was considered likely metastatic given its solitary appearance and the absence of features suggesting primary lung malignancy, although histologic confirmation was required for staging. Combined CO2 laser-assisted supraglottic partial laryngectomy and video-assisted thoracoscopic surgery wedge resection of the right upper lobe was therefore planned for airway protection, curative-intent resection with negative margins, and staging confirmation. Neck dissection was considered a conditional component, to be reassessed based on intraoperative frozen section. Intraoperatively, malignancy was confirmed on pulmonary frozen-section analysis, establishing M1 disease. At this point, platinum-etoposide systemic chemotherapy was anticipated as the treatment backbone regardless of histologic subtype. Given NEC’s biological similarity to small cell lung cancer (in which widely metastatic disease is not surgically curable), and timely initiation of systemic therapy is the principal determinant of outcome [7,8], the added surgical burden of neck dissection was judged likely to delay systemic therapy without commensurate oncologic benefit. Neck dissection was not performed; cervical lymph node management was deferred to systemic therapy.
Final histopathology of the supraglottic specimen confirmed NEC, small cell type, with nests of small cells showing high mitotic activity; immunohistochemistry was positive for CD56, synaptophysin, and TTF-1, focally positive for p63, negative for chromogranin A, with Ki-67 of 40%-50% (Fig. 9). The pulmonary specimen was a poorly differentiated carcinoma with neuroendocrine features and focal squamous differentiation (metastasis vs. synchronous primary), showing focal TTF-1, p40, and p63 positivity with CD56 and synaptophysin negativity, plus lymphovascular emboli and spread through air spaces. Both resection margins were negative (supraglottic 0.1 cm, pulmonary <0.1 cm). Although differing marker profiles precluded pathology-based confirmation, the lesion was clinically interpreted as metastatic based on 1) absent primary lung features, 2) shared neuroendocrine differentiation, and 3) the known propensity of head and neck NEC for early distant metastasis.

Histopathology of Case 2. Supraglottic partial laryngectomy specimen showing NEC, small cell type, diffusely composed of nests of small cells with high mitotic activity and crushing artifacts (A: hematoxylin and eosin [H&E] ×200), and diffuse positive immunohistochemical staining for synaptophysin (B: immunohistochemistry ×200). NEC, neuroendocrine carcinoma.
Postoperatively, six cycles of palliative cisplatin-etoposide achieved complete response. Subsequent surveillance revealed recurrence at the left level III node and two new pulmonary nodules; palliative radiotherapy (5500 cGy each to the neck and lung over 1 month) was followed by second-line FOLFIRI. The primary surgical site remained free of recurrence at 6 months (Fig. 6B). The patient continues on systemic therapy. The detailed treatment course and response evaluation over a 21-month follow-up period are summarized in Table 2.
This study was approved by the Institutional Review Board of Korea University Ansan Hospital (IRB No. 2026AS0058), and informed consent was waived.
Discussion
The 2022 WHO classification distinguishes well-differentiated NETs (G1-G3) from poorly differentiated NECs (small cell and large cell types) [3]. Former terms such as “well-differentiated NEC” and “moderately differentiated NEC” are now classified as NET G1 and G2, respectively (Table 1) [3,9].
In both cases, synaptophysin and CD56 were consistently positive, whereas chromogranin A was absent or only focal—characteristic of NECs rather than NETs [3]. Ki-67 of 80% (Case 1) and 40%-50% (Case 2) confirmed the diagnosis. Case 1 showed mixed large and small cell features; Case 2 was predominantly small cell type with crushing artifacts [3,10].
Because NEC is morphologically indistinguishable from poorly differentiated or non-keratinizing SCC—particularly in small biopsies—a combined panel of neuroendocrine and squamous markers is essential. Diffuse synaptophysin and CD56 positivity with a high Ki-67 supports NEC, whereas consistent p40 or cytokeratin 5/6 expression favors SCC [4]. Our cases met these criteria, with absent or focal squamous markers (p40 negative in Case 1; p63 focal in Case 2) allowing unambiguous NEC classification. Notably, p16 was focally positive in Case 1 and diffusely positive in Case 2. Although p16 overexpression is classically linked to human papillomavirus (HPV)-driven oropharyngeal SCC, it also occurs in head and neck NECs irrespective of HPV status and does not confer a favorable prognosis [11-13]. Because NEC diagnosis was already established morphologically and immunohistochemically, p16 did not alter classification—illustrating that p16 must be interpreted within the full marker context to avoid misclassifying NEC as HPV-related SCC, which carries different prognostic and therapeutic implications. HPV-specific testing was not performed; however, given the unequivocal neuroendocrine morphology, HPV status would not have altered diagnosis or treatment.
A practical challenge in head and neck NEC is the absence of a dedicated tumor, node, metastasis (TNM) staging system. In Case 2, the tumor would have been staged T2N1M1 under the American Joint Committee on Cancer (AJCC) SCC system; no NEC-specific staging exists, making prognostication less standardized than for SCC [2,14].
The meta-analysis of 436 laryngeal NEC cases showed superior survival with chemoradiotherapy over surgery alone (5-year disease-specific survival: 31% vs. 13%), while surgery with neck dissection was effective for NETs [7,8]. Platinum-etoposide is the treatment backbone for NEC; surgery is considered selectively for symptom control or histological confirmation.
NEC of the head and neck follows a systemic disease biology analogous to small cell lung cancer, with early hematogenous spread and high distant failure rates despite aggressive locoregional control. Both cases illustrate this. In Case 1, extensive metastases precluded surgery, and palliative carboplatin-etoposide was administered. In Case 2, surgery addressed airway risk and confirmed pulmonary metastasis; upon intraoperative M1 confirmation, systemic chemotherapy was prioritized over further locoregional intensification. While curative-intent metastasectomy and neck dissection are established in oligometastatic SCC, this paradigm does not extrapolate to NEC given its systemic biology. The subsequent locoregional recurrence in Case 2 required salvage radiotherapy and second-line chemotherapy, reflecting NEC’s aggressive biology.
A systematic review of oropharyngeal NEC confirmed high rates of early distant metastasis despite locoregional control [15], underscoring the importance of early comprehensive staging with PET-CT.
In conclusion, head and neck NEC is a rare but aggressive malignancy requiring immunohistochemical diagnosis, PET-CT staging, and individualized multidisciplinary treatment. Dedicated staging systems and treatment guidelines remain to be established.
Notes
Acknowledgments
This research was supported by a grant of the MD-PhD/Medical Scientist Training Program through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea.
Author Contribution
Conceptualization: Soon Young Kwon. Data curation: Dorjsuren Tsagaankhuu, Jeonghwan Kim. Investigation: Dorjsuren Tsagaankhuu, Jeonghwan Kim, Jung-Woo Choi. Supervision: Soon Young Kwon. Validation: Soon Young Kwon. Writing—original draft: Dorjsuren Tsagaankhuu, Jeonghwan Kim. Writing—review & editing: Jung-Woo Choi, Soon Young Kwon.