žĄú Ž°†
Merkel žĄłŪŹ¨ŽäĒ žßĄŪĒľ Žāīžóź ž°īžě¨ŪēėŽäĒ žč†Í≤ĹŽāīŽ∂ĄŽĻĄžĄłŪŹ¨(neuroendocrine cell) ž§Ď ŪēėŽāėžĚīŽč§. Merkel žĄłŪŹ¨žēĒžĚÄ 1972ŽÖĄ Toker [1]žóź žĚėŪēī ž≤ėžĚĆ žÜĆÍįúŽźėžóąžúľŽ©į ŽįĪŽßĆ Ž™ÖŽčĻ 4Ž™Ö ž†ēŽŹĄžĚė ŽįúžÉĚŽ•†žĚĄ ÍįĞߥ ŽďúŽ¨ł žēÖžĄĪžĘÖžĖĎžúľŽ°ú ž£ľŽ°ú 60ŽĆÄ žĚīžÉĀžĚė Í≥†Ž†ĻžóźžĄú ŽįúžÉĚŪēúŽč§. žĘÖžĖĎžĚÄ ž†Ąž≤īžĚė 50%ÍįÄ ŽĎźÍ≤ĹŽ∂Ğ󟞥ú ŽįúžÉĚŪēėŽäĒŽćį, žôłžĚīŽŹĄžóź ŽįúžÉĚŪēú Í≤ĹžöįŽäĒ ž†Ą žĄłÍ≥Ąž†ĀžúľŽ°ú Žß§žöį ŽďúŽ¨ľÍ≤Ć Ž≥īÍ≥†ŽźėÍ≥† žěąŽč§[2,3].
ŪĎúž§Ä žĻėŽ£ĆŽäĒ žēĄžßĀÍĻĆžßÄ ž†ēŽ¶ĹŽźėžßÄ žēäžēėžúľŽāė žėĀžó≠Ž¶ľŪĒĄž†ąŽ°úžĚė ž†ĄžĚīŽāė žõźÍ≤© ž†ĄžĚī ŽįŹ žě¨ŽįúžĚī ŽĻąŽ≤ąŪēėÍ≤Ć ŽįúžÉĚŪēėžó¨ ÍĶ≠žÜĆž†ąž†úŽßĆžúľŽ°úŽäĒ Ž∂ąž∂©Ž∂ĄŪēėŽč§ŽäĒ žĚėÍ≤¨žĚī žöįžõĒŪēėŽč§. Kokoska ŽďĪ[4]žĚÄ 35Ž™ÖžĚė ŪôėžěźŽ•ľ ŽĆÄžÉĀžúľŽ°ú 31ÍįúžõĒÍįĄ ž∂Ēž†Ā ÍīÄžįįžĚĄ žčúŪĖČŪēėžėĞ̥ ŽēĆ ÍĶ≠žÜĆž†ąž†úžôÄ Ūē®ÍĽė žėąŽį©ž†Ā Í≤ĹŽ∂Äž†ąž†úžą†, žąėžą† ŪõĄ Žį©žā¨žĄ†žĻėŽ£ĆŽ•ľ Ūē®ÍĽė žčúŪĖČŪēėžó¨ ÍĶ≠žÜĆ ŽįŹ žõźÍ≤© žě¨ŽįúžĚĄ Žāģž∂ĒÍ≥† žÉĚž°īžú®žĚĄ ŽÜížĚłŽč§Í≥† Ž≥īÍ≥†ŪēėžėÄŽč§. Žč§Ž•ł žóįÍĶ¨žóźžĄúŽŹĄ 181Ž™ÖžĚė ŪôėžěźŽ•ľ ŽĆÄžÉĀžúľŽ°ú ÍĶ≠žÜĆž†ąž†úžą†žĚĄ žčúŪĖČŪēú ŪôėžěźžóźžĄú ÍĶ≠žÜƞ쨎įúžĚī ŪĚĒŪēėŽč§ŽäĒ Í≤įÍ≥ľŽ•ľ Ž≥īžėÄŽč§. žĚīž≤ėŽüľ ŽĆÄŽ∂ÄŽ∂ĄžĚė ŪôėžěźžóźžĄú žąėžą† ŪõĄ Žį©žā¨žĄ†žĻėŽ£ĆŽ•ľ Ž≥ĎŪĖČŪēėŽ©į, ÍīĎŽ≤ĒžúĄŪēú ž†ąž†úžôÄ Žį©žā¨žĄ†žĻėŽ£ĆžóźŽŹĄ Ž∂ąÍĶ¨ŪēėÍ≥† 1ŽÖĄ žÉĚž°īžú®žĚÄ 85%, 5ŽÖĄ žÉĚž°īžú®žĚÄ 62%, 10ŽÖĄ žÉĚž°īžú®žĚÄ 47%Ž°ú Ž≥īÍ≥†Žźú ŽįĒ žěąŽč§[5].
ž†ÄžěźŽď§žĚÄ žôłžĚīŽŹĄžóź ÍĶ≠ŪēúŽźú Merkel žĄłŪŹ¨žēĒžĘ֞󟞥ú ÍĶ≠žÜĆž†ĀžĚł ž†ąž†úžąėžą† Žč®ŽŹÖ žčúŪĖČ ŪõĄ žě¨Žįú žóÜžĚī Í≤ĹÍ≥ľ ÍīÄžįį ž§ĎžĚł ž¶ĚŽ°Äžóź ŽĆÄŪēėžó¨ Ž¨łŪóĆ Í≥†žįįÍ≥ľ Ūē®ÍĽė Ž≥īÍ≥†ŪēėŽäĒ ŽįĒžĚīŽč§.
ž¶Ě Ž°Ä
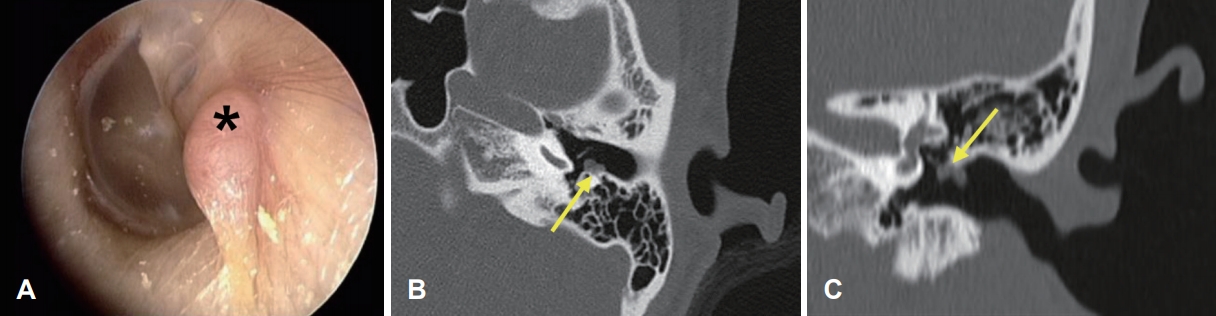
32žĄł žó¨žěź ŪôėžěźÍįÄ Žāīžõź 2ÍįúžõĒ ž†Ą žöįžóįŪěą ŽįúÍ≤¨Žźú žĘĆžł° žôłžĚīŽŹĄžĚė žĘÖÍīīŽ•ľ ž£ľžÜĆŽ°ú ŽāīžõźŪēėžėÄŽč§. Í≥ľÍĪįŽ†•žúľŽ°ú Žāīžõź 44ÍįúžõĒ ž†Ą ÍįĎžÉĀžĄ† žú†ŽĎźžÉĀžēĒ žßĄŽč®Ūēė ÍįĎžÉĀžĄ† ž†Ąž†ąž†ú žąėžą†žĚĄ ŽįõžēėŽč§. Í∑Ä ŽāīžčúÍ≤Ĺ Í≤Äžā¨žóźžĄú žĘĆžł° žôłžĚīŽŹĄ ŪõĄŽį©žóź 3√ó2 mmžĚė ŪĀ¨ÍłįžĚė Ž∂ČÍ≥† ÍĶ¨žßĄžÉĀžĚė žĘÖŽ¨ľžĚī žěąžóąžúľŽ©į(Fig. 1A), ž£ľžúĄ ž°įžßĀžĚīŽāė Í≤ĹŽ∂Äžóź ž†ĄžĚīŽ•ľ žĚėžč¨Ūē†ŽßĆŪēú ŪäĻŽ≥ĄŪēú žÜĆÍ≤¨žĚÄ ÍīÄžįįŽźėžßÄ žēäžēėŽč§. žł°ŽĎźÍ≥® ž†ĄžāįŪôĒŽč®žłĶžī¨žėĀžóźžĄú žĘĆžł° žôłžĚīŽŹĄžóź ŪŹīŽ¶ĹžĖĎžÉĀžĚė žóįž°įžßĀ žĘÖŽ¨ľ ŪôēžĚłŽźėžóąžúľŽ©į, Í≥®žĻ®Ž≤Ē žÜĆÍ≤¨žĚÄ ÍīÄžįįŽźėžßÄ žēäžēėŽč§(Fig. 1B and C). žąúžĚĆ ŽįŹ žĖīžĚĆž≤≠ÍįĀÍ≤Äžā¨, žěĄŪĒľŽćėžä§ ž≤≠Ž†•Í≤Äžā¨ Í≤įÍ≥ľŽäĒ ž†ēžÉĀžĚīžóąŽč§.
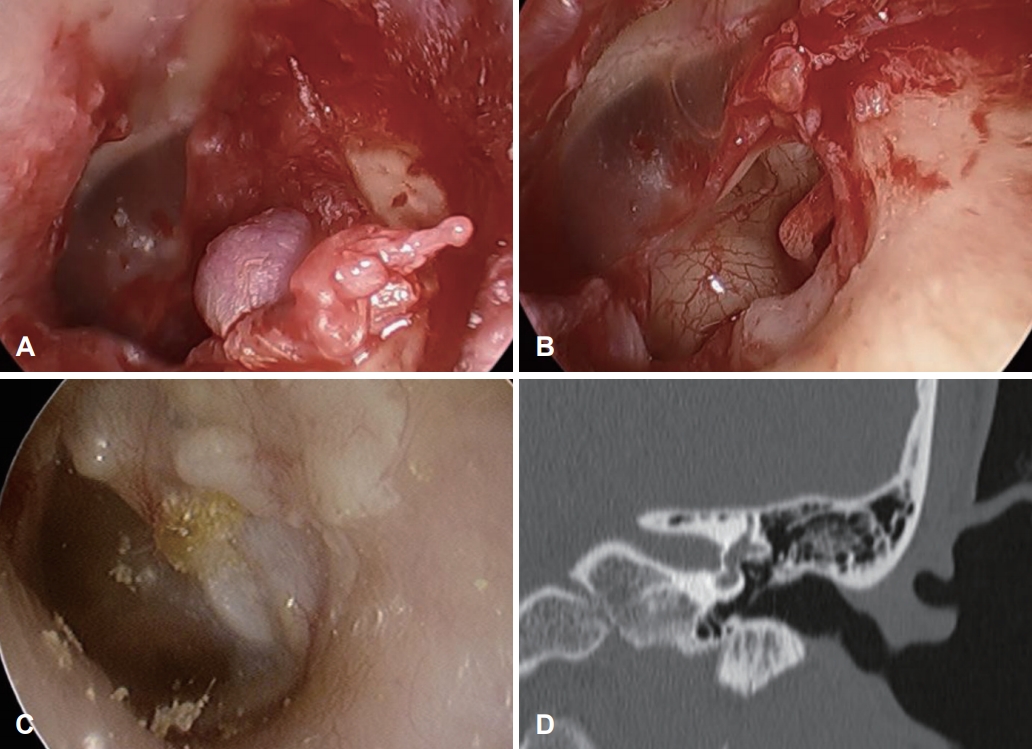
žÉĀÍłį Í≤įÍ≥ľŽ•ľ Ū܆ŽĆÄŽ°ú Í≤ĹÍ≥ĄÍįÄ Ž∂ĄŽ™ÖŪēėÍ≥† žĻ®žäĶž†ĀžĚīžßÄ žēäžĚÄ žĖĎžĄĪ žĘÖžĖϞ̥ žĚėžč¨ŪēėžėÄÍ≥†, ž°įžßĀÍ≤Äžā¨žôÄ žĘÖžĖĎ ž†úÍĪįŽ•ľ Ūē®ÍĽė žčúŪĖČŪēėÍłį žúĄŪēī ŽāīžčúÍ≤Ş̥ žĚīžö©Ūēú ž†ąž†úžÉĚÍ≤Ğ̥ žčúŪĖČŪēėžėÄŽč§(Fig. 2A). žąėžą† žčú žĘÖŽ¨ľžĚÄ Žč®Žč®ŪēėžėÄÍ≥† Í≥†ŽßȞ̥ ŪŹ¨Ūē®Ūēú ž£ľžúĄžóź Í≥†ž†ēŽźú žÉĀŪÉúŽ°ú Í≥†ŽßČžĚė žĚľŽ∂ÄŽ•ľ ŪŹ¨Ūē®Ūēėžó¨ ž†ąž†úžÉĚÍ≤Ğ̥ žčúŪĖČŪēėžėÄŽč§. ž†ąž†úŪēú ž°įžßĀžĚÄ 3√ó2 mm ŪĀ¨ÍłįžĚė Í≤ĹÍ≥ĄÍįÄ Ž™ÖŪôēŪēú žĘÖžĖĎžĚīžóąžúľŽ©į ŽāīžčúÍ≤Ĺ žÜĆÍ≤¨žóźžĄú ž£ľŽ≥Ä ž°įžßĀžúľŽ°úžĚė žĻ®žú§žĚīŽāė žĚīžÜĆÍ≥® ŽėźŽäĒ žēąŽ©īžč†Í≤ĹžúľŽ°úžĚė žĻ®Ž≤ĒžĚÄ Ž≥īžĚīžßÄ žēäžēėŽč§.
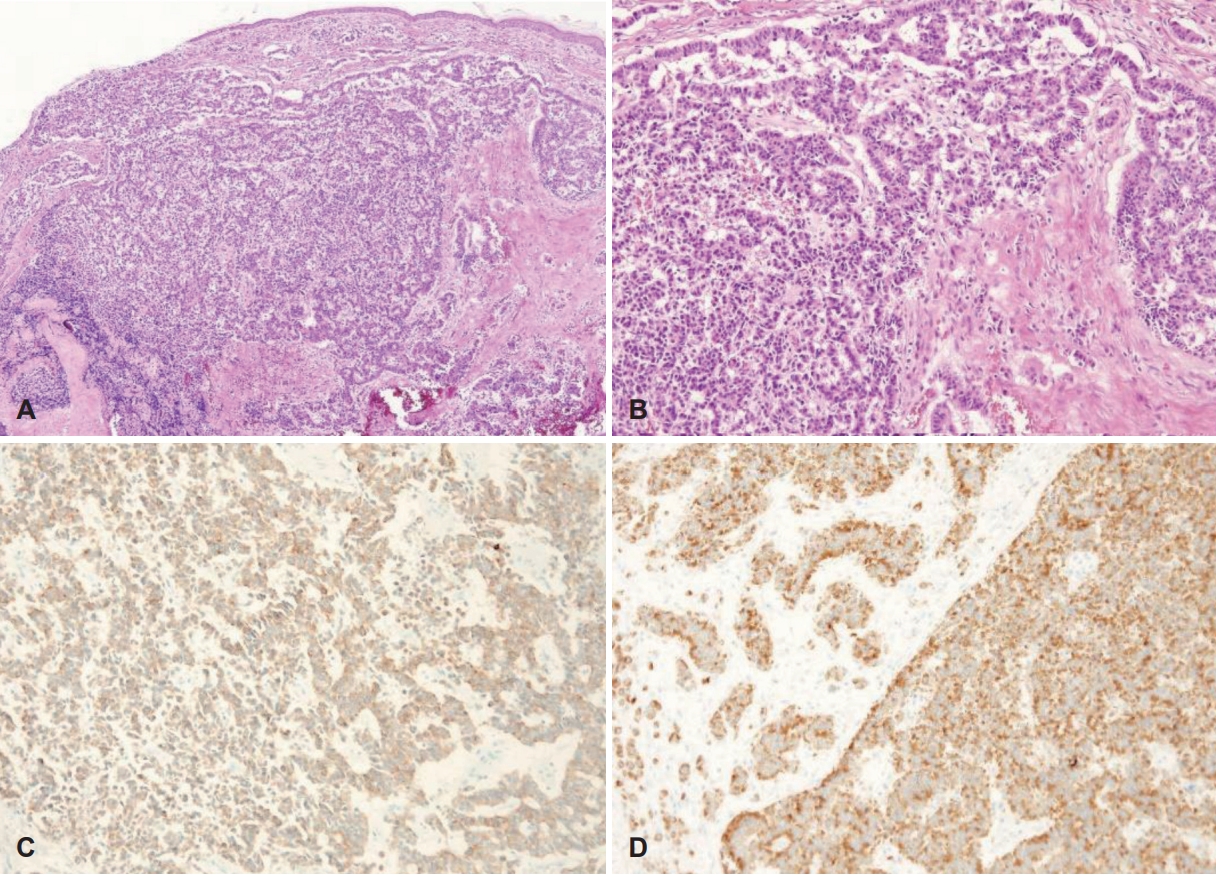
Ž≥ĎŽ¶¨ž°įžßĀŪēôž†Ā Í≤Äžā¨ Í≤įÍ≥ľ žôłžĚīŽŹĄžóźžĄú ÍłįžõźŪēú žĘÖžĖĎžĚī Í≥†žč§Ž•úžĚĄ žĻ®Ž≤ĒŪēėžėÄžúľŽ©į žĄłŪŹ¨žßąžĚī ž†ĀžĚÄ ŪĎłŽ•łŽĻõžĚė žěĎÍ≥† ŽĎ•Í∑ľ žĄłŪŹ¨Žď§žĚī žßĄŪĒľžóź ŪĆźžÉĀ(sheet) ŪėĻžĚÄ žĄ¨žú†ž£ľ(trabecular) ŪėēŪÉúžĚė ÍĶ¨ž°įŽ•ľ žĚīŽ£®Í≥† žěąŽäĒ žĖĎžÉĀžĚĄ Ž≥īžėÄŽč§. žĚīŽü¨Ūēú žĘÖžĖĎžĄłŪŹ¨ŽäĒ cytokeratin 20(CK20)žóź ŽĆÄŪēú Ž©īžó≠ž°įžßĀŪôĒŪēôžóľžÉȞ󟞥ú žĘÖžĖĎžĄłŪŹ¨ ŪēĶ ž£ľŽ≥ÄžúľŽ°ú ž†źžÉĀžĚė žĖĎžĄĪŽįėžĚϞ̥ Ž≥īžĚīŽ©į, syneptophysin žóľžÉČ žó≠žčú žĖĎžĄĪ žÜĆÍ≤¨žĚĄ Ž≥īžó¨ Merkel žĄłŪŹ¨žēĒžúľŽ°ú ŪôēžßĄŽźėžóąŽč§(Fig. 3).
žąėžą† ŪõĄ žčúŪĖČŪēú žěźÍłįÍ≥ĶŽ™ÖžėĀžÉĀžóźžĄú žěĒž°īŪēėŽäĒ žĘÖŽ¨ľ ŽįŹ ž£ľžúĄ žěĄŪĆĆžĄ†žúľŽ°úžĚė ž†ĄžĚī žÜĆÍ≤¨žĚīŽāė žĖĎž†ĄžěźŽį©ž∂úŽč®žłĶžī¨žėĀžóźžĄú ŪÉÄ žě•ÍłįŽ°úžĚė ž†ĄžĚī žÜĆÍ≤¨žĚÄ ÍīÄžįįŽźėžßÄ žēäžēĄ the American Joint Committee on Cancer(AJCC) Ž≥ĎÍłįž≤īÍ≥ĄžÉĀ 1Íłįžóź ŪēīŽčĻŪēėžėÄŽč§. žĘÖžĖĎžĚī Žß§žöį žěĎÍ≥† ž£ľžúĄ ž°įžßĀÍ≥ľžĚė Í≤ĹÍ≥ĄÍįÄ Ž∂ĄŽ™ÖŪēėÍ≤Ć ž†úÍĪįŽźėžĖī ž∂ĒÍįÄž†ĀžĚł Žį©žā¨žĄ†žĻėŽ£ĆŽäĒ ŪēėžßÄ žēäžēėžúľŽ©į 41ÍįúžõĒÍįĄ žč†ž≤īÍ≤Ğߥ ŽįŹ žěźÍłįÍ≥ĶŽ™ÖžėĀžÉĀžóźžĄú žě¨ŽįúžÜĆÍ≤¨ žóÜžĚī ž∂Ēž†Ā ÍīÄžįį ž§ĎžĚīŽč§(Fig. 2C).
Í≥† žįį
Merkel žĄłŪŹ¨ŽäĒ žßĄŪĒľ ŽāīžóźžĄú ŪäĻžąėÍįźÍįĀÍłįÍīÄžĚė žó≠Ūē†žĚĄ ŪēėŽäĒ žĄłŪŹ¨Ž°úžĄú, žĄłŪŹ¨žßą Žāīžóź melanin Í≥ľŽ¶ĹÍ≥ľ žč†Í≤Ĺž†ĄŽč¨ Í≥ľŽ¶ĹžĚĄ ÍįÄžßÄÍ≥† žěąžĖī Í∑ł ÍłįžõźžĚĄ žč†Í≤ĹŽ¶ČžĚė žôłŽįįžóĹž§ĄÍłįžĄłŪŹ¨ŽĚľÍ≥† ž∂Ēž†ēŪēėÍ≥† žěąŽč§. Merkel žĄłŪŹ¨žēĒžĚÄ Žß§žöį ŽďúŽ¨ł ŪĒľŽ∂ÄžĚė žč†Í≤ĹŽāīŽ∂ĄŽĻĄ žēĒžĘÖžúľŽ°ú žēĆŽ†§ž†ł žěąžúľŽ©į, 1972ŽÖĄ Toker [1]žóź žĚėŪēī ž≤ėžĚĆžúľŽ°ú žßÄž£ľ žēĒžĘÖ(trabecular carcinoma)žĚīŽĚľ Ž™ÖŽ™ÖŽźėžĖī Ž≥īÍ≥†ŽźėžóąŽč§.
Ž≥īÍ≥†žóź ŽĒįŽĚľ Žč§žÜĆ žį®žĚīÍįÄ žěąžúľŽāė ž†Ąž≤īžĚė žēĹ 50% žĚīžÉĀžĚī ŽĎźÍ≤ĹŽ∂Ğ󟞥ú ŽāėŪÉÄŽāėŽ©į ŪėĎŽ∂Ä, ŽĻĄŽ∂Ä, žēąÍĶ¨ ž£ľžúĄžóź ŪėłŽįúŪēúŽč§. 60~70ŽĆÄžĚė Í≥†Ž†Ļžóź ŽįúžÉĚŪēėÍ≥† ŪŹČÍ∑† žóįŽ†ĻžĚÄ 69žĄłŽ°ú Ž≥īÍ≥†ŽźėÍ≥† žěąžúľŽ©į, ž£ľŽ°ú ŽįĪžĚłžĘÖžóź ŪėłŽįúŪēėŽ©į žĄĪŽ≥Ąžóź ŽĒįŽ•ł ŽįúžÉĚžĚė žį®žĚīŽäĒ ŪĀ¨žßÄ žēäžúľŽāė žóįÍĶ¨žóź ŽĒįŽĚľ žį®žĚīŽ•ľ Ž≥īžĚłŽč§[6]. žôłžĚīŽŹĄžóźžĄú ÍłįžõźŪēú Merkel cell carcinomaŽäĒ ž†ĄžĄłÍ≥Ąž†ĀžúľŽ°ú Žß§žöį ŽďúŽ¨ľÍ≤Ć Ž≥īÍ≥†ŽźėÍ≥† žěąžúľŽ©į, ŪŹČÍ∑† 69žĄłžĚė Í≥†Ž†ĻžĚė ŪôėžěźžóźÍ≤ĆžĄú ŽįúŽ≥ĎŪēėŽäĒŽćį Ž≥ł ž¶ĚŽ°Ä ŪôėžěźŽäĒ 32žĄłŽ°ú ŪĚĒŪēėžßÄ žēäžĚÄ ŪĚ•ŽĮłŽ°úžöī ž¶ĚŽ°ÄžĚīŽč§.
žĶúÍ∑ľ ŽįúŽ≥ĎŽ•†žĚÄ ž¶ĚÍįÄŪēėŽäĒ ž∂ĒžĄłŽ°ú 1986~2001ŽÖĄÍĻĆžßÄ žóįŽ†ĻžĚĄ Ž≥īž†ēŪēú ŽįúŽ≥ĎŽ•†žĚÄ 8% ž¶ĚÍįÄŪēėžėÄžúľŽ©į[7], ŽĄ§ŽćúŽěÄŽďúžóźžĄúŽŹĄ 1993~1997ŽÖĄ žā¨žĚī ŽįĪŽßĆ Ž™ÖŽčĻ 1.7Ž™ÖžóźžĄú 2003~2007ŽÖĄ žā¨žĚī 3.5Ž™ÖžúľŽ°ú ŽįúŽ≥ĎŽ•†žĚī ž¶ĚÍįÄŪēėžėÄŽč§[8]. ž†ĄžĚīžôÄ žě¨ŽįúŽŹĄ ŪĚĒŪēėÍ≤Ć ŽāėŪÉÄŽāė 25%~30%žĚė ŪôėžěźžóźžĄú žě¨ŽįúžĚī ŽāėŪÉÄŽāėŽ©į ÍĶ≠žÜĆž†ĄžĚīŽäĒ 52%~59%, žõźÍĪįŽ¶¨ ž†ĄžĚīŽäĒ 34%~36%Ž°ú Ž≥īÍ≥†ŽźėžóąŽč§. žěĄžÉĀž†Ā Ž≥ĎÍłįžóź ŽĆÄŪēīžĄúŽäĒ žĶúÍ∑ľÍĻĆžßÄŽŹĄ ž†ēŽ¶ĹŽźėžßÄ žēäžēĄ žßÄŽāú 20ŽÖĄÍįĄ 5ÍįÄžßÄžĚė ž≤īÍ≥ĄÍįÄ ž†úžēąŽźėžóąžúľŽ©į AJCCžóźžĄú 2018ŽÖĄ ž†úžēąŪēú Ž≥ĎÍłįž≤īÍ≥ĄžôÄ Í∑łžóź ŽĒįŽ•ł 5ŽÖĄ žÉĚž°īžú®žĚÄ Žč§žĚĆÍ≥ľ ÍįôŽč§(Table 1).
žěĄžÉĀž†ĀžúľŽ°ú žąėž£ľžóźžĄú žąėÍįúžõĒÍįĄ ŽĻ†Ž•īÍ≤Ć ž¶ĚÍįÄŪēėŽäĒ Ž∂ČžĚÄ Ž≥īŽěŹŽĻõžĚė Žč®Žč®Ūēú Í≤įž†ēžĄĪ žĘÖÍīīŽ°ú Žß§ŽĀĄŽü¨žöįŽ©į ÍīĎŪÉĚžĚī žěąŽäĒ ŪĎúŽ©īžĚĄ Ž≥īžó¨[9] Ž≥ł ž¶ĚŽ°ÄžĚė žßĄžįį žÜĆÍ≤¨Í≥ľ žĚľžĻėŪēėžėÄŽč§. Ž≥ł ž¶ĚŽ°ÄžóźžĄúŽäĒ žöįžóįŪěą ŽįúÍ≤¨Žźú žôłžĚīŽŹĄ žĘÖÍīīŽ•ľ ž£ľžÜĆŽ°ú ŽāīžõźŪēėžó¨ ŪôėžěźÍįÄ ŪėłžÜĆŪēėŽäĒ ŪäĻžĚī ž¶ĚžÉĀžĚī žóÜžóąžúľŽāė Í≤Ĺžöįžóź ŽĒįŽĚľ Ž¨īŪÜĶžĄĪžĚė žĘÖÍīīžôÄ Ūē®ÍĽė ž†ĄžĚĆžĄĪ Žāúž≤≠žĚĄ Ž≥īžĚľ žąė žěąžúľŽ©į žÜĆžĖĎÍįź, ÍįĄŪ󟞆Ā žĚīŪÜĶ ŽįŹ žąėžĖĎžĄĪ Ž∂ĄŽĻĄŽ¨ľžĚĄ ŪėłžÜĆŪē† žąė žěąŽč§[3].
Merkel žĄłŪŹ¨žēĒžĚė ŪĎúž§Ä žĻėŽ£ĆŽäĒ žõźÍ≤©ž†ĄžĚīÍįÄ žóÜŽäĒ ŪôėžěźžóźžĄúŽäĒ žĘÖžĖϞ̥ žôĄž†Ąž†ąž†úŪēėŽäĒ Í≤ÉžĚīŽč§. ž†ąž†úžóįžúľŽ°úŽ∂ÄŪĄį 2~3 cmÍĻĆžßÄ ŪŹ¨Ūē®Ūēėžó¨ ž†ąž†úŪēėŽäĒ Í≤ÉžĚī ž∂Ēž≤úŽźėŽ©į, ÍīĎŽ≤ĒžúĄŪēú ž†ąž†úžą†žĚĄ žčúŪĖČŪēú Í≤Ĺžöįžóź Ž¨īŽ≥ĎžÉĚž°īžú®(disease free survival)žĚĄ ÍįúžĄ†žčúŪā®Žč§Í≥† Ž≥īÍ≥†Žźú ŽįĒ žěąŽč§[4]. žėąŽį©ž†ĀžĚł Í≤ĹŽ∂Ä Ž¶ľŪĒĄž†ą Í≥Ĺž≤≠žą†žĚÄ žą†žěźžóź ŽĒįŽĚľ Žč§Ž•īÍ≤Ć ž†Āžö©ŽźúŽč§. ŪėĄžě¨ÍĻĆžßÄŽäĒ Ž¶ľŪĒĄž†ą ž†ĄžĚīÍįÄ žóÜŽäĒ ŪôėžěźŽäĒ žēĹ 15%~20%žóź Ž∂ąÍ≥ľŪēėŽĮÄŽ°ú ž†Ąžč† žĽ®ŽĒĒžÖėžĚī žĖĎŪėłŪēėŽč§Ž©ī žĄ†ŪÉĚž†Ā Í≤ĹŽ∂Ä Ž¶ľŪĒĄž†ą Í≥Ĺž≤≠žą†žĚĄ žĻėŽ£Ćžóź ŪŹ¨Ūē®Ūēīžēľ ŪēúŽč§ŽäĒ žĚėÍ≤¨žĚī ŽĆÄž≤īž†ĀžĚīŽāė[10], Žč§Ž•ł žóįÍĶ¨žóźžĄúŽäĒ 1 cm ŽĮłŽßĆžĚė žěĎžĚÄ Ž≥ĎŽ≥Ğ󟞥úŽäĒ ÍĶ≠žÜĆ Ž¶ľŪĒĄ ž†ĄžĚīžĚė ÍįÄŽä•žĄĪžĚī ŽāģžēĄ žĄ†ŪÉĚž†Ā Í≤ĹŽ∂Ä Ž¶ľŪĒĄž†ą Í≥Ĺž≤≠žą†žĚī ŪēĄžöĒ ŪēėžßÄ žēäŽč§Í≥† ž†úžēąŪēėÍłįŽŹĄ ŪēėžėÄŽč§[11]. ÍĶ≠žÜĆ Žį©žā¨žĄ†žĻėŽ£ĆÍįÄ žąėžą† žĚīŪõĄžĚė žě¨Žįú, ž†ĄžĚīŽ•ľ Žāģž∂ėŽč§ŽäĒ Í≤ÉžĚī ŽßéžĚÄ žóįÍĶ¨Ž•ľ ŪÜĶŪēėžó¨ Ž≥īÍ≥†ŽźėžóąžúľŽ©į[12], žĚľŽ∂Ğ󟞥úŽäĒ Žį©žā¨žĄ† žĻėŽ£ĆŽ•ľ Žč®ŽŹÖžúľŽ°ú žčúŪĖČŪēėŽäĒ Í≤ɞ̥ ž£ľžě•ŪēėÍłįŽŹĄ ŪēėžėÄžúľŽāė Íłįž°īžĚė ÍīĎŽ≤ĒžúĄž†ąž†úžą†Í≥ľ Žį©žā¨žĄ†žĻėŽ£ĆŽ•ľ Ūē®ÍĽė žčúŪĖČŪēú ŽĆÄž°įÍĶįžóź ŽĻĄŪēėžó¨ žú†žĚėŪēú žĚīŽď̞̥ Ž≥īžĚīžßÄ žēäžēėŽč§[13]. Ūē≠žēĒžĻėŽ£ĆŽäĒ žě¨ŽįúžĚīŽāė žõźÍĪįŽ¶¨ ž†ĄžĚīÍįÄ žěąŽäĒ Í≤Ĺžöį žôĄŪôĒŽ™©ž†ĀžúľŽ°ú žā¨žö©ŽźėŽäĒ Í≤ÉžĚī žĚľŽįėž†ĀžĚīŽ©į Merkel žĄłŪŹ¨žēĒžóź ŪäĻžĚīž†ĀžĚł ŪĎúž§Ä Ūē≠žēĒžĻėŽ£ĆŽäĒ ž†ēŽ¶ĹŽźėžßÄ žēäžēĄ žĄłŪŹ¨Ūēôž†Ā žú†žā¨žĄĪžĚĄ Í≥†Ž†§Ūēėžó¨ žÜĆžĄłŪŹ¨ŪŹźžēĒÍ≥ľ žú†žā¨ŪēėÍ≤Ć žĻėŽ£ĆŪēúŽč§. Merkel žĄłŪŹ¨žēĒžóź ŪäĻžĚīž†ĀžĚł ŪĎúž†ĀžĻėŽ£ĆÍįÄ žóįÍĶ¨ž§ĎžĚīŽ©į žĶúÍ∑ľ Merkel cell polyomavirus (MCV)ÍįÄ Ž≥ĎŪÉúžÉĚŽ¶¨žóź ÍīÄžó¨ŪēúŽč§ŽäĒ žóįÍĶ¨Í≤įÍ≥ľŽ•ľ ÍłįŽįėžúľŽ°ú žĚīŽ•ľ žĚīžö©Ūēú Ž©īžó≠ ž°įž†ą žĻėŽ£ĆÍįÄ ž†úžčúŽźėÍ≥† žěąŽč§. Merkel cell carcinomažôÄ MCVžĚė ÍīÄÍ≥ĄŽäĒ žēĄžßĀ ž∂©Ž∂ĄŪěą ŽįĚŪėÄžßÄžßÄ žēäžēėžúľŽāė MCVžĚė TŪē≠žõźžĚī short hairpin RNA(shRNA)Ž•ľ Žß§ÍįúŽ°ú Ūēėžó¨ žĄłŪŹ¨žĄĪžě•Í≥ľ žā¨Ž©łžĚĄ ž°įž†ąŪēėŽäĒ Í≥ľž†ēžóźžĄú Merkel cell carcinomažĚė ŽįúžÉĚžóź Íłįžó¨ŪēėŽäĒ Í≤ÉžúľŽ°ú žÉĚÍįĀŽźėŽ©į Ūē≠ŽįĒžĚīŽü¨žä§ Ūö®Í≥ľÍįÄ žěąŽäĒ interferon-őĪ, ő≤ ŽďĪžĚī Merkel cell carcinomažĚė žĻėŽ£Ćžóź ž†úžēąŽźėÍłįŽŹĄ ŪēėžėÄŽč§[14].
Ž≥ł ž¶ĚŽ°ÄžóźžĄúŽäĒ žąėžą† ž†Ą žßĄžįįžÜĆÍ≤¨ ŽįŹ žėĀžÉĀÍ≤Äžā¨žóźžĄú Í≤ĹÍ≥ĄÍįÄ Ž™ÖŪôēŪēėŽ©į žĻ®žäĶž†ĀžĚīžßÄ žēäžĚÄ žĖĎžĄĪ žĘÖžĖĎžĚī žĚėžč¨ŽźėžĖī ž°įžßĀÍ≤Äžā¨žôÄ žôĄž†Ąž†ąž†úŽ•ľ Ūē®ÍĽė žčúŪĖČŪēėŽäĒ žąėžą†ž†Ā žĻėŽ£ĆŽ•ľ žčúŪĖČŪēėžėÄŽč§. Ž≥ĎŽ¶¨ž°įžßĀŪēô Í≤Äžā¨žóźžĄú Merkel cell carcinomaŽ°ú žĶúžĘÖ žßĄŽč®ŽźėžóąžúľŽāė žĘÖžĖĎžĚė ŪĀ¨ÍłįÍįÄ 1 cm ŽĮłŽßĆžúľŽ°ú Žß§žöį žěĎÍ≥† žąėžą† ž†ĄŪõĄžĚė žßĄžįįžÜĆÍ≤¨Í≥ľ žėĀžÉĀÍ≤Äžā¨žóźžĄú ž†ĄžĚī žÜĆÍ≤¨žĚĄ Ž≥īžĚīžßÄ žēäžēėžúľŽ©į Í≤ĹÍ≥ĄÍįÄ Ž™ÖŪôēŪēėÍ≤Ć ž†úÍĪįŽźėžĖī ž∂ĒÍįÄ Í≤ĹŽ∂Ä ž†ąž†úžą† ŽįŹ Žį©žā¨žĄ†žĻėŽ£ĆŽäĒ žčúŪĖČŪēėžßÄ žēäžēėžúľŽ©į ž†ēÍłįž†ĀžĚł žč†ž≤īžßĄžįį ŽįŹ žěźÍłįÍ≥ĶŽ™ÖžėĀžÉĀÍ≤Äžā¨Ž•ľ ŪÜĶŪēėžó¨ žě¨Žįú žó¨Ž∂ÄŽ•ľ ž∂Ēž†Ā ÍīÄžįįŪēėÍ≥† žěąŽč§. žĚīž≤ėŽüľ žěĄžÉĀž†Ā Ž≥ĎÍłįÍįÄ ŽāģžĚÄ Merkel cell carcinomaŽäĒ ÍĶ≠žÜĆž†ąž†úžąėžą† Žč®ŽŹÖ žčúŪĖČŽßĆžúľŽ°úŽŹĄ žĘčžĚÄ žėąŪõĄŽ•ľ Ž≥īžĚľ žąė žěąŽč§ŽäĒ ž†źžĚĄ žčúžā¨Ūēėžó¨ Ž¨łŪóĆ Í≥†žįįÍ≥ľ Ūē®ÍĽė Ž≥īÍ≥†ŪēėŽäĒ ŽįĒžĚīŽč§.